Count on This System to Find MDM Level
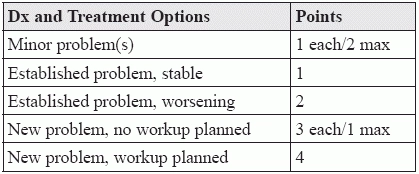
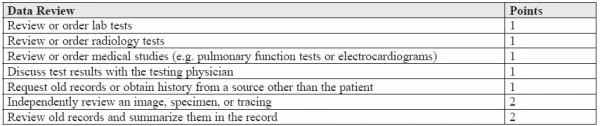
Points system helps take guesswork out of complexity determination. As important as medical decision making (MDM) is for determining the level of E/M documented, even experienced coders know finding the precise complexity of MDM is as much an art as it is a science. That’s why “CMS distributed a point system for MDM originally developed by the Marshfield Clinic to Medicare carriers to be used on a voluntary basis,” according to Mary I. Falbo, MBA, CPC, CEO of Millennium Healthcare Consulting Inc. in Lansdale, Pennsylvania. But does the MDM point system create more problems than it solves? We asked some experienced coders this question, and here’s what they had to say. How the Problem and Data Points Add Up Like CPT® guidelines, the scoring system breaks MDM down into three components: the number of diagnoses or management options involved; the amount or complexity of data to be reviewed; and the degree of risk associated with the patient’s conditions, the diagnostic procedures, or management options. What’s different is that the scoring system assigns points for the diagnosis and treatment options and the data review. The following tables show how you assign the points: For both MDM components, scores totaling one point would indicate the MDM involved was straightforward, two points would equate to a low complexity, three would lift the complexity level to moderate, and four or more would indicate a high level of MDM complexity. Assign an Appropriate Level of Risk The last component of MDM, the level of risk, is the only one not scored. Instead, you pick one element from the patient’s presenting problems, the provider’s orders for diagnostic procedures, and options your provider selects for management to help you determine the highest level. The highest level of risk in any one of these three categories determines whether the overall risk is minimal, low, moderate, or high. (To determine risk, you’ll need to consult a chart such as the one CMS provides at www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/Downloads/eval-mgmt-serv-guide-ICN006764.pdf.) Coding Caution As easy as all this sounds, “determining risk level is where the gray areas come in, as there are several items that can impact your decision,” warns Chelle Johnson, CPMA, CPC, CPCO, CPPM, CEMC, AAPC Fellow, billing/credentialing/auditing/coding coordinator at County of Stanislaus Health Services Agency in Modesto, California. “Items such as the number of conditions, whether they are acute or chronic, whether the drugs are prescription or over the counter, and so on can all change the leveling of MDM,” Johnson continues. Putting it all Together Finally, you plot the highest levels of each component on a grid like the following to determine the overall complexity of MDM: For a given level of MDM complexity, you must score two out of three among problem points, data points, and risk. For instance, high MDM complexity requires at least two of the following: 4 problem points, 4 data points, and/or a high level of risk. So, your provider diagnoses a patient with a previous history of polycystic ovary syndrome with a new problem — acute abdominal pain with rebound tenderness. The provider orders a lab test to evaluate for sepsis, IV hydromorphone for pain management, and imaging to rule out an appendectomy or other abdominal pathology before sending the patient to the nearest emergency department. Based on this scenario, you would assign four problem points for the new problem and planned workup, one point for ordering the lab, and assign a high risk level based on the decision to order the IV hydromorphone — a parenteral controlled substance. As only two of the three components are necessary to assign MDM complexity, and as the problem points and risk levels are the highest possible, this would lead you to assign a high MDM complexity level to this encounter. But, Johnson notes, whether your office uses the system to code encounters like this or not, it is important to be aware that the system is not perfect. “The system still leaves a lot of gray areas that can become battlegrounds during audits,” Johnson warns. For instance, a patient that previously had diabetes and now has diabetes with nephropathy could be regarded as having an established problem that’s worsening or as having a new problem. For that reason, Johnson believes, your office should have clear policies in place regarding those gray areas. “That way, if you are audited, you will be able to show consistency in your determinations,” Johnson argues. Additionally, “even though you may use the point system to justify the E/M level your provider has performed, the most important factor in determining the appropriate level is medical necessity,” Falbo cautions. “Even if there is a large amount of documentation to justify the choice, the E/M level must match the patient’s condition and the treatment options that it necessitates,” Falbo concludes.