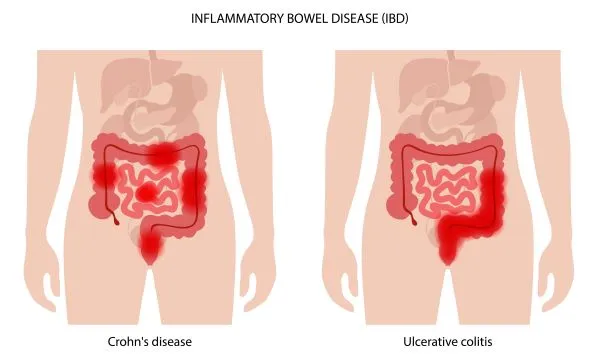
Decipher the Differences Between Crohn’s and Ulcerative Colitis
Learn the anatomy of the code sets for each condition. Inflammatory bowel disease (IBD) is a term that can include several different diagnoses, most commonly, Crohn’s disease and ulcerative colitis. How you code these diagnoses and the symptoms associated with them depends on the physician’s notes as well as some general knowledge of how each code set is organized. The coding for the two conditions is pretty straight forward once you know how the code sets are broken down. Here, we’re going to outline the similarities and differences between the two conditions and how to code them. Identify the Conditions that Make Up IBD IBD is a general term that encompasses conditions involving immune response and inflammation of the GI tract, such as Crohn’s disease and ulcerative colitis. IBD is not to be confused with irritable bowel syndrome (IBS), however. Where IBD is an autoimmune condition, IBS is a functional disorder, meaning it causes symptoms but doesn’t cause visible inflammation or actual damage to the digestive tract. Also, IBD diagnoses generally require imaging or colonoscopies, whereas a physician can generally diagnose IBS based on symptoms and the exclusion of other conditions. Crohn’s disease: Crohn’s disease involves chronic inflammation of almost any part of the gastrointestinal tract, though it most commonly affects the small intestine and colon. Also known as regional enteritis, the disease causes symptoms including: Ulcerative colitis: Ulcerative colitis affects the colon primarily, and it affects only the lining of the colon. Here again, the patient may complain of similar symptoms, and possibly also R15.2 (Bowel urgency). Note: Although symptoms of Crohn’s and ulcerative colitis are similar, Crohn’s disease can occur anywhere between the mouth and the anus, while ulcerative colitis occurs only in the colon. Also, “Crohn’s disease can cause inflammation that may go all the way through the layers of the intestine, unlike ulcerative colitis, which is basically a disease of the mucosa, the inner lining,” explains Glenn D. Littenberg, MD, MACP, FASGE, AGAF, a gastroenterologist and former CPT® Editorial Panel advisor for ASGE in Pasadena, California. Coding for ulcerative colitis and Crohn’s disease may pose challenges as there are so many options available to pick from. Here is how to simplify the coding conundrums and reach the precise code once you have identified the needful information from your providers’ notes. Know the Anatomy of the Codes There are 28 code options for Crohn’s and 49 for ulcerative colitis. Symptoms and anatomical position of symptoms are key. These are the details you need to know in order to accurately code both conditions with the greatest specificity: Location: Essentially, the first four characters for any of the codes for Crohn’s disease and ulcerative colitis have to do with location as described by the physician. Here are a few examples: Note the differences: The GI tract is a complicated place, and the physician may not use the words “small intestine.” The ICD-10 section for K50- lists synonyms which should help you correctly categorize. For example, if the Crohn’s disease is in the duodenum, ileum, or jejunum, you’ll categorize the condition as occurring in the small intestine. Synonyms for K50- also include regional ileitis and terminal ileitis, “which refers to the very last portion of small intestine and junction with the colon at the ileocecal valve, a very common area of Crohn’s involvement,” says Littenberg. Also: These conditions can occur in the large and small intestine simultaneously. Because Crohn’s disease and ulcerative colitis occur in different part so the body, the code sets for each will not be parallel. K50.9 (Crohn’s disease of both small and large intestine…) does not have an ulcerative colitis counterpart. Remember, ulcerative colitis appears only in the colon. Existence of complications: The fifth character signifies whether there are complications, as seen from these two codes: Specific complication: Once you have checked the notes for any specific complication, you’ll apply a sixth character to describe it, whether you’re coding Crohn’s or ulcerative colitis. The pattern looks like this: Note that, because the pathology of Crohn’s disease often involves a deep extent of inflammation, an obstruction, fistula or abscess is much more likely to be a manifestation of Crohn’s disease than of ulcerative colitis. Applying the sixth character, then, will lead you to such codes as: Remember: Under both K50- and K51- you’ll find an Excludes1 note for the other, which means you cannot report both conditions on the same claim. See also the Use Additional note and code any manifestations if applicable. Understand the Evolutionary Nature of Each Condition Both Crohn’s disease and ulcerative colitis can evolve over time. In other words, the areas of involvement identified initially may change. A patient with Crohn’s disease of the large intestine may later be found to have small intestine involvement also. It is not unusual for the diagnosis codes to change depending on the patient’s symptoms and the findings. Additionally, it is even possible that what appeared to be a pathology-confirmed diagnosis of ulcerative colitis initially will, at a future time, be more consistent with Crohn’s disease. Do not be surprised if your physician uses a different diagnosis for the patient’s condition from visit to visit depending on the current signs, symptoms, and radiologic or colonoscopic findings. As always: If you don’t see either condition specifically mentioned, then the inflammation could be from a different etiology, such as ischemic colitis, microscopic colitis, infectious colitis, or drug-related side-effects. “If ever it’s unclear which diagnosis to code based on the documentation, it’s necessary to query the provider,” says Laidy Martinez, CPC, CGIC, CASCC, profee coder at Children’s Health of Orange County in Orange County, California.