Get Ready to Take a Giant Leap Forward in Moderate Sedation Coding
Learn the ins and outs of 99152 vs. GMMM1, and more.
Wondering what codes to report when you administer moderate sedation in 2017? The American Medical Association’s (AMA) Current Procedural Terminology (CPT®) editorial panel created separate CPT® and HCPCS codes in for reporting of moderate sedation services in 2017. Clear up your endoscopy coding conundrums with a quick rundown on must-know facts and tips.
Wake Up to These New Moderate Sedation Codes in 2017
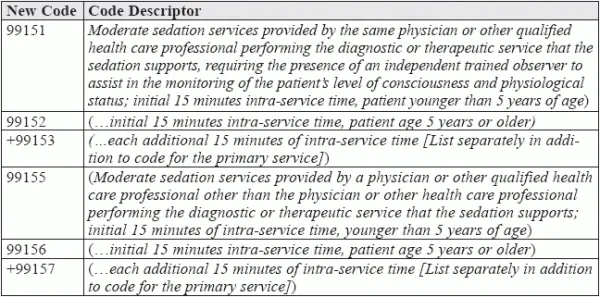
The prior moderate (conscious) sedation codes (99143-99150) have been deleted and replaced with new codes in 2017. Now providers who perform their own moderate sedation with a procedure must report the appropriate new moderate sedation code (99151-99157) to receive full payment. “This change will impact gastroenterology providers’ bottom line with less reimbursement,” says Catherine Brink, BS, CMM, CPC, CMSCS, CPOM, president, Healthcare Resource Management, Inc. Spring Lake, NJ. On a similar note, “from the provider’s prospective, this will not be a good thing, as this will directly impact the amount of RVUs they bring in with each scope,” says Lisa Center, CPC, Physician Practice Manager, Via Christi Hospital Pittsburg, Inc. Pittsburg, KS.
Time: The biggest change is that the intraservice time thresholds have dropped from 30 minutes to 15 minutes. In 2016, the primary conscious sedation codes 99143, 99144, 99148, and 99149 all represented the first 30 minutes of intraservice time. CPT® 2016 add-on codes +99145 and +99150 covered each additional 15 minutes. “In 2017, the add-on codes for each additional 15 minutes are +99153 and +99157,” says Michael Weinstein, MD, former representative of the AMA’s CPT® Advisory Panel. “The change to 15 minute intervals is more typical for standard anesthesia billing units.”
Pull the Plug on an Endoscopy Exclusive Sedation Code: GMMM1
What’s more, now you have an exclusive new HCPCS code GMMM1 (Moderate sedation services provided by the same physician or other qualified health-care professional performing a gastrointestinal endoscopic service [excluding biliary procedures] that sedation supports, requiring the presence of an independent trained observer to assist in the monitoring of the patient’s level of consciousness and physiological status; initial 15 minutes of intra-service time, patient age 5 years or older) for all endoscopic procedures during which moderate sedation is inherent to the procedure (except a few, as we shall see below).
The reason: CMS published proposed RVUs for the new moderate sedation CPT® codes in the CY 2017 PFS. However, as the gastroenterological societies’ survey data were significantly different from other specialties, CMS created a new code GMMM1.
Payors on the new codes: The new moderate sedation CPT® codes will be recognized by all payors. However, code GMMM1 for physicians who perform gastroenterology endoscopy procedures will apply only to Medicare. You will need to contact your payors to find out if they will be acknowledging GMMM1 for reimbursement in 2017.
Learn Which Codes Go With GMMM1 and 99152
For the Medicare program, CMS proposed that administration of moderate sedation for the following CPT® and HCPCS codes, be reported using GMMM1, which describes the first 15 minutes of intra-service time:
On the other hand, to report the intraservice administration of moderate sedation for the following endoscopic retrograde cholangiopancreatography (ERCP) procedures and dilation codes you may use 99152, which describes the first 15 minutes of intra-service time:
What if there was no sedation? If your provider performs endoscopic or esophageal dilation procedure without any sedation, only report the appropriate procedure code (43213, 43214, 43233, 43450, or 43453). Do not report moderate sedation code 99152 or GMMM1 in addition to the procedure code.
What Does Intraservice Time Mean? Find Out
This is important to understand because as you need to report only the intraservice time in the required time threshold for each code descriptor. For an endoscopic procedure, you would count the intraservice time as the “scope-in to scope-out” portion of the service provided. It begins at the insertion of the first scope and ends at the removal of the last scope. It does not include face-to-face time with the patient prior to the procedure, or at the conclusion of the procedure once the provider removes the scope and stabilizes/transfers the patient to the recovery unit.
To capture the first 15 minutes of intra-service time, use GMMM1 or 99152. Report the add-on code 99153 for each additional 15 minutes of intra-service time beyond the first 15 minutes. However, because time-based CPT® codes apply when at least half of the listed time is achieved, you can report+99153 only when the intra-service time runs longer than next eight minutes.
Example: For reporting an endoscopic procedure with an intra-service time of 23 minutes use one unit of GMMM1 and one unit of 99153, even though the provider could not fulfill 15 minutes of additional intra-service time.
Final takeaway: “The change in the coding methodology for endoscopic procedures is unlikely to change the sedation method used by your physician,” says Weinstein. “If they performed many of their procedures in the past with anesthesiologist or CRNA assistance, then they will probably continue working in that fashion. The procedure value change of 0.1 RVU will result in a $3-4 drop per case. If they have typically administered their own sedation during procedures, then they will likely continue and will now receive additional reimbursement depending on the length of the case.”
To know more go to https://www.gastro.org/practice-management/reimbursement/2017_MPFS_Proposed_Rule_Moderate_Sedation_-_Q-A.pdf.