Shore Up Pediatric UTI Coding
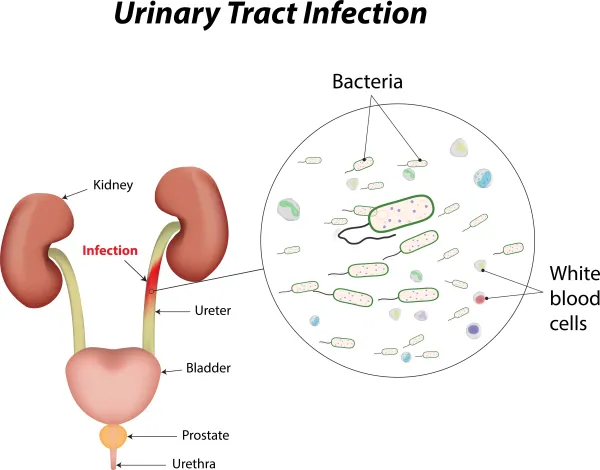
Keep these tips handy for this common diagnosis. Urinary tract infections (UTIs) are common in infants and children, according to the American Acadaemy of Pediatrics. In fact, approximately 3 percent of girls and 1 percent of boys will have a UTI by 11 years of age. Although girls are diagnosed with UTIs more frequently than boys, uncircumcised boys have slightly more diagnoses of UTIs than those who have been circumcised. (Source: www.healthychildren.org/English/health-issues/conditions/genitourinary-tract/Pages/Detecting-Urinary-Tract-Infections.aspx). Make sure you’re coding this common condition correctly. Refer to the following guidance, which includes the most used diagnostic codes for pediatric UTI encounters, as well as some expert tips. Beware of these Issues with N39.0 On the surface, coding for a UTI seems simple, as there is only one code that goes by that name: N39.0 (Urinary tract infection, site not specified). “The choice may be attractive and the obvious choice to the provider. However, there are a couple of issues with this,” says Donna Walaszek, CCS-P, billing manager, credentialing/coding specialist for Northampton Area Pediatrics LLP, in Northampton, Massachusetts. Problem 1: N39.0 is an “unspecified” code, and this lack of specificity presents a real problem for reimbursement because “the industry is moving toward diagnostic-based reimbursement, so the use of unspecified codes is becoming less accepted and diagnosing a UTI without a culture is becoming a thing of the past,” Walaszek cautions. This means you’ll have to dig a little deeper into the ICD-10 index, which lists several other related conditions that your pediatrician could use. Problem 2: N39.0, along with several other codes from the Diseases of the Genitourinary System chapter of ICD-10 that may come into play, features a note that tells you to use an additional code from B95-B97 to identify the infectious agent, if applicable, after your provider has administered a test. This also becomes a problem because “the likelihood that a provider has the resources, in house, to identify the infectious agent to meet coding guidelines is pretty slim, leading the provider to code based on the presenting signs and symptoms,” says Walaszek. “As such, I recommend coding based on signs and symptoms if the provider is unable to meet the coding guidelines requiring an infectious agent,” Walaszek advises. Dive Deeper into Signs and Symptoms “While a provider is in the process of forming a formal UTI diagnosis, you might use diagnosis codes from Chapter 18, Symptoms, Signs and Abnormal Clinical and Laboratory Findings Not Elsewhere Classified,” suggests JoAnne M. Wolf, RHIT, CPC, CEMC, coding manager at Children’s Health Network in Minneapolis. “Two that immediately come to mind are R30.9 [Painful micturition, unspecified] for painful urination or R32 [Unspecified urinary incontinence] for urinary incontinence,” Wolf adds. Even though these signs and symptoms are also unspecified, they are still the best codes to use in the absence of a definitive diagnosis. Other codes that could come into play at this point of your provider’s evaluation of the condition could also include codes from R33.- (Retention of urine), R35.- (Polyuria), or R39.1- (Other difficulties with micturition). Nail Location for Definitive Dx “Once the provider makes a formal UTI diagnosis, the provider should use the specific site if known,” Wolf advises. That means narrowing the diagnosis based on the location of the infection by consulting the chart below to locate the correct code or group. You will also need to pay close attention to your provider’s note to see if the patient has been diagnosed with acute (sudden) or chronic (persistent) cystitis. If your pediatrician has documented that the patient has acute cystitis, you’ll report N30.0- (Acute cystitis), but if the documentation states the patient’s cystitis is chronic, you’ll report N30.1- (Interstitial cystitis (chronic)) or N30.2- (Other chronic cystitis). Don’t Miss These Important Exceptions Your pediatrician could also possibly use one of three other codes to indicate that the patient has a UTI. Two of them N99.521 (Infection of incontinent external stoma of urinary tract) and N99.531 (Infection of continent stoma of urinary tract) are codes that describe infections that affect the urinary tract following a surgery, such as a urostomy, that involves creating a stoma, or opening, in a patient’s body to remove bodily waste. Before using one of these codes, however, you will need to make sure that your physician has documented and confirmed a cause-and-effect relationship between the procedure and the condition. Lastly, “if the patient is under 28 days of age and has a UTI, you will need to use P39.3 [Neonatal urinary tract infection],” Wolf reminds coders.