Concentrate on Severity While Coding Asthma With J45

Hint: Identify symptoms and medication use for accurate reporting.
When your internist diagnoses asthma, you’ll have to focus more on the severity of the condition to accurately report the diagnosis with ICD-10 codes rather than paying attention to the etiology as you need to do when reporting this condition using the ICD-9 system of codes.
ICD-9: When reporting a diagnosis of acute exacerbation of asthma using ICD-9 codes, you will have to focus on etiology of the condition to accurately report it. When your internal medicine physician arrives at a diagnosis of acute exacerbation of asthma, you will have to start with 493 (Asthma).
Depending on the causative factor for the asthma, 493 will expand into the following five codes:
The codes 493.0, 493.1, 493.2, and 493.9 further expand using a fifth digit depending on the asthma state into unspecified, status asthamaticus, and acute exacerbation.
For example, 493.0 expands into the following three codes:
493.8 expands into these two codes:
ICD-10: When ICD-10 codes come into effect, 493 under ICD-9 codes will crosswalk to J45 (Asthma). But, unlike ICD-9 codes, your ICD-10 coding is not centered over the etiology of the condition but follows the severity of the symptoms and the necessity for treatment with a nebulizer.
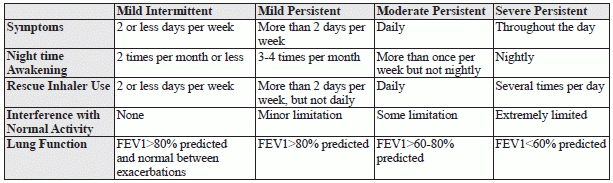
Based on severity, you have the following four states of the condition (see chart for details):
When using ICD-10 codes, you will have to delve into the documentation to assess the severity of the condition as this is necessary for accurate reporting. J45 will further expand, based on severity, into the following five code sets:
All these above mentioned codes further expand based on the asthma state into uncomplicated, acute exacerbation, and status asthamaticus.
For example, J45.2 expands into the following three subsets:
Example: Your internist assesses an established patient with asthma who is currently experiencing episodes of acute exacerbation. Your physician records a detailed history that reveals that the patient has been suffering from increasing incidence of symptoms that is now increased to episodes of wheezing on a daily basis. He is also experiencing the symptoms during the night and that is awakening him more than once a week but not on a daily basis. The acute exacerbation of symptoms has been limiting his daily activities to a certain extent.
On questioning, he tells your internist that his use of the inhaler has increased, and since he has episodes of wheezing every day, he seems to be using the inhaler on a daily basis. Your internal medicine specialist reviews the patient’s utilization of the inhaler and seeks to determine if he has been using the device properly, to check in case misuse has been the cause for his increase in symptoms.
Your internist orders some pulmonary function tests. He records a forced expiratory volume in 1 second (FEV1) >70%. Based on the symptoms and results of tests, your physician infers that the patient is suffering from acute exacerbation of a moderate persistent type of asthma.
What to report: You report the evaluation of the patient with an appropriate evaluation and management code (E/M), such as 99213 (Office or other outpatient visit for the evaluation and management of an established patient, which requires at least 2 of these 3 key components…);the evaluation of the patient’s use of the MDI with 94664 (Demonstration and/or evaluation of patient utilization of an aerosol generator, nebulizer, metered dose inhaler or IPPB device). Don’t forget to provide documentation to support the 94464 to let the payer know that your internist performed the evaluation to know if the device was being used properly as he was trying to assess the cause for the increase in symptoms. You may also want or need to append modifier 25 to the E/M code to reflect that it was significant and separately identifiable from the evaluation done as part of 94664.
You report the diagnosis using J45.41 (Moderate persistent asthma with [acute] exacerbation) if you are using ICD-10 codes or use 493.92 (Asthma, unspecified, with (acute) exacerbation) if you are using the ICD-9 coding system.