Monitor Wandering Before You Code
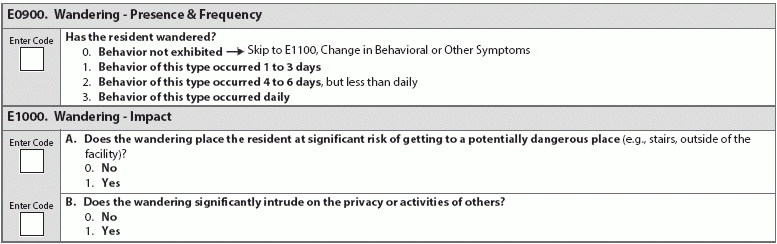
Evaluate the awareness and safety of the resident before coding Section E. With the updates to Section P (Restraints and Alarms) and surveyors' promise to enforce new and existing rules to curb antipsychotic use, you may be wondering how to keep some residents who are prone to wandering safe without risking compliance issues. One of the most significant aspects of evaluating, care planning, and coding wandering is the determination of the cause. Top tip: Nurse Assessment Coordinators and team staff should pay special attention in assessing residents who were admitted to the facility after close calls due to wandering. Take note: Some researchers' definitions of wandering directly contradict the RAI Manual's guidance. This contradiction means that a behavior noted on a resident's chart may not be consistent with the coding requirements of the MDS. Myra A. Aud, PhD, RN, concludes that there are four specific types of wandering, in her paper "Dangerous wandering: elopements of older adults with dementia from long-term care facilities": However: The RAI Manual provides these explicit instructions on page E-18, which exclude pacing. The RAI Manual provides guidance on wandering: Top tip: Many of the behaviors that are associated with or because wandering may also involve delirium, dementia, adjustments to new medications or dosages or contraindications. Make sure you are assessing and documenting those variables as well, both in the clinical record and in the MDS. Monitor Wandering to Keep Residents Safe The RAI Manual notes that not all wandering behaviors are harmful, but staff should keep an eye on residents so they don't end up in unsafe situations. Really consider all of the possibilities and contingencies here; for example, a wandering male resident who enters female residents' rooms could be unintentionally subjecting the other residents to harassment. This kind of behavior would definitely qualify as a significant disruption to other residents and would need to be documented accordingly in item E1000B (Wandering Impact, Does the wandering significantly intrude on the privacy or activities of others?). Make Care Plans Comprehensive and Individualized Care plans should focus on safety - of both the wandering resident and everyone else. If the wandering resident is known to use their hands to seek out door knobs, etc., take extra care that unoccupied wheelchairs' brakes are always locked, and make sure medication carts or equipment areas are always secured or completely inaccessible. Care plans should be focused on minimizing the wandering issue, which means determining and addressing any root causes, and employing proactive and reactive steps. Staff should know the best way to respond to an active wandering situation, including the best practices for each individual resident, if intervention is necessary. Take steps to limit the access and range of wandering residents, including door alarms and door barriers. Even - perhaps especially - residents who are in a locked unit may be prone to wandering behaviors. Code E0900 (Wandering – Presence & Frequency) like this: Code 0, behavior not exhibited: if wandering was not exhibited during the 7-day look-back period. Skip to E1100 (Change in Behavioral or Other Symptoms). Code 1, behavior of this type occurred 1-3 days: if the resident wandered on 1-3 days during the 7-day look-back period, regardless of the number of episodes that occurred on any one of those days. Proceed to answer E1000 (Wandering – Impact). Code 2, behavior of this type occurred 4-6 days, but less than daily: if the resident wandered on 4-6 days during the 7-day look-back period, regardless of the number of episodes that occurred on any one of those days. Proceed to answer E1000 (Wandering – Impact). Code 3, behavior of this type occurred daily: if the resident wandered daily during the 7-day look-back period, regardless of the number of episodes that occurred on any one of those days. Proceed to answer E1000 (Wandering – Impact). Coding Instructions for E1000A(Does the Wandering Place the Resident at Significant Risk of Getting to a Potentially Dangerous Place?): Code 0, no: if wandering does not place the resident at significant risk. Code 1, yes: if the wandering places the resident at significant risk of getting to a dangerous place (e.g., wandering outside the facility where there is heavy traffic) or encountering a dangerous situation (e.g., wandering into the room of another resident with dementia who is known to become physically aggressive toward intruders). Coding for e1000B (Does the wandering significantly intrude on the privacy or activities of others?) Code 0, no: if the wandering does not intrude on the privacy or activity of others. Code 1, yes: if the wandering intrudes on the privacy or activities of others (i.e., if the wandering violates other residents' privacy or interrupts other residents' performance of activities of daily living or limits engagement in or enjoyment of social or recreational activities), whether or not the other resident complains or communicates displeasure or annoyance.