
Don't Get Burned When Reporting Burn Cases
Tip: Focus on degree and percentage affected.
An insight to types of burns and a summarization of 4-step procedure to code your burned cases will help in smooth reimbursement process.
Dig Into the Depth and Degree of Burn
There are six degrees of burns, based on severity. We’ll focus on first- and second-degree burns and coding, as they are relevant in an outpatient setting.
Calculate The Body Surface Area
The degree of burn is not enough to determine your coding. You need to categorize burns by the percentage of body area affected as well. For example, “he has a second-degree burn over 45 percent of his body” is a typical way to report a burn case.
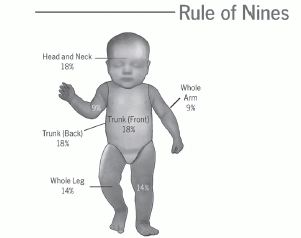
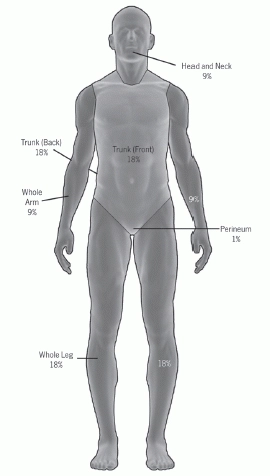
Know “The Rule Of Nines”
Percentages of burn are essentially defined by using “The Rule of Nines.” Hence a good idea is to know this rule, which is essential for CPT® coding of second-degree and higher burn cases.
Take note: A child’s body area is measured in a different way than an adult. The reason is that the baby’s head and torso have more skin than their appendages. A second-degree burn of a small child, even at a lower percentage of skin area, presents a greater risk and requires more emergency care as compared to an adult with the same type of burn.
Each area of the body has a percentage amount assigned, and all the percentage amounts added together equal 100 percent (see Rule of Nines illustrations for percentage breakdown).
Focus on Degree of Burn While Documenting
As mentioned earlier, your physician must document the degree of the burn and the percentage of body area affected before you can bill accurately. For second-degree burns, it is essential to include a description of the management or treatment rendered during the visit. This is important because burn coding can be done for both dressing changes and debridement.
Correctly Code For Burn Cases
Knowing the following codes would help you to use appropriate codes for different procedures used to manage burn cases.
Typical procedure codes include:
16000 Initial treatment, first degree burn, when no more than local treatment is required.
Code 16000 is used for initial treatment while codes 16020, 16025, and 16030 are for initial and subsequent visits.
Take note: Paying attention to these following points would help you bill burn cases accurately:
Pinpoint the Best Diagnosis:
Once you determine the best procedure code, it’s time to choose the most accurate diagnosis. Refer to the “Injury and Poisoning” section of ICD-9-CM codes for burns, found in the range 940-949 (except for sunburn which is reported with 692.7) Burn codes from 940-946 involve specific body areas, including multiple sites.
Pay attention: Special instructions go with code 948 for “burns classified according to extent of body surface involved.” The ICD-9-CM codebook instructs, “This category is to be used when the site of the burn is unspecified, or with categories 940-947 when the site is specified.” The code requires a fifth digit if the burn is third degree.
E code Precision: Apart from the diagnosis and procedure codes describing the type of burn and body area, a variety of E codes may be used to describe how the injury occurred. For example, E958.1 (Suicide and self-inflicted injury by burns fire), E968.0 (Assault by fire), and E988.1 (Injury by burns or fire undetermined whether accidentally or purposely inflicted) are all burns due to fire. A burn caused by a hot liquid in an assault is coded to E968.3 (Assault by hot liquid).
Practice With This Case Study
Scenario: A wheelchair-bound patient came to the clinic after dropping a pot of boiling tea onto her lap. She had second-degree burns on both upper legs (anterior and posterior) and on the genital area. Areas are dressed with Silvadene™ cream and bandages. Patient is prescribed medication for pain and is asked to come back after three days for possible debridement, along with dressing change.
Step 1: Calculate the percentage of the area burned. Total both upper legs for 18 percent (9 percent for the upper portion of each leg) and add an additional 1 percent for the genital area. A total of 19 percent of body area is affected.
Step 2: Assign the procedure code. You need to use code 16030 (Dressings and/or debridement of partial-thickness burns.....), as these are partial thickness burns covering more than one extremity or 10 percent of body area. An evaluation and management (E/M) code in the 9920x-9921x series is also appropriate when appended with modifier 25 (Significant, Separately Identifiable Evaluation and Management Service by the Same Physician on the Same Day of the Procedure or Other Service), depending upon the documentation.
Step 3: Choose the diagnosis code. The appropriate diagnosis codes for our example above, for instance, would be:
Step 4: Check for an E code. You can report the incident using E924.0 (Accident caused by hot substance or object, caustic or corrosive material, and steam; hot liquids and vapors, including steam).
16020 Dressings and/or debridement of partial-thickness burns, initial or subsequent; small (less than 5% total body surface area).
16025 Dressings and/or debridement of partial-thickness burns, initial or subsequent; medium (e.g., whole face or whole extremity, or 5% to 10% of total body surface area).
16030 Dressings and/or debridement of partial-thickness burns, initial or subsequent; large (e.g., more than 1 extremity, or greater than 10% of total body surface area).
