CPT® 2016 Makes These 7 Key Ob-Gyn Updates

Ovarian sclerotherapy changes will get your attention.
While the October change to ICD-10 is grabbing a lot of headlines right now, the annual updates to CPT® won’t be far behind. Here’s a seven-part breakdown of what will be headed your way for implementation in January 2016.
1. Acquaint Yourself With This New Ovarian Sclerotherapy Code
As of January 1, you will have the following new code to represent ovarian sclerotherapy:
“This procedure would be performed on women with endometriomas as an alternative to open or laparoscopic surgery,” says Melanie Witt, CPC, COBGC, MA, an independent coding consultant in Guadalupita, N.M.
What happens: Ovarian sclerotherapy uses ultrasound-guided aspiration with a sclerosing agent such as 95% ethanol (EST) or methotrexate. The purpose of the sclerosing agent (irritant) is to prevent ovarian cyst regrowth by chemically destroying the wall of the cyst. This treatment option is less invasive than laparoscopic surgery and takes approximately 20–30 min to perform.
Sclerotherapy, unlike other treatment options, is less likely to damage healthy ovarian tissue and, it is hoped will be less likely to reduce the number of ovum still in the ovary. Risks associated with sclerotherapy include infection, internal bleeding, and irritation from the sclerosing agent. To reduce irritation, the agent is removed after 10 min, and the pelvic area is rinsed with saline.
2. Fixate On These New Fetal MR Codes
You’ll have these two fetal MRI codes:
Fetal MR is indicated when:
1. An abnormality on ultrasound is not clearly defined and more information is needed to make a decision about therapy, delivery, or to advise the parents about prognosis. An example of when this might apply is when there is maternal obesity, oligohydramnios, or advanced gestational age, Witt says.
2. An abnormality is identified on ultrasonography and the treating physician wants MR-specific information in order to make decisions about care. An example might include the calculation of MR-derived fetal lung volumes in cases of congenital diaphragmatic hernia.
3. A fetus is significantly at risk for abnormality that will affect prognosis — even if no finding is discovered with ultrasound (e.g., the fetus could develop neurologic ischemia after laser ablation of connecting blood vessels between the twins in Twin-Twin Transfusion Syndrome [TTTS]).
3. Master This Screening Mammography Revision
77057 Screening mammography, bilateral (2-view film study of each breast)
In 2016, you’ll have a subtle change for this mammography code:
Emphasis on this change is film replaced by the word “study.” “The number of films taken does not impact the use of the code,” Witt says.
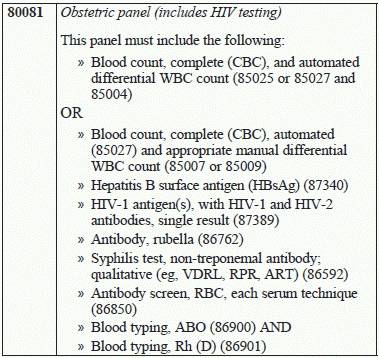
4. Here’s How 80081 Will Become Your New OB Panel Code
You will have a new option for an obstetric panel, which is:
Your current obstetric panel is 80055 (Obstetric panel), and this panel must include the following:
OR
The difference is the inclusion of “HIV-1 antigen(s), with HIV-1 and HIV-2 antibodies, single result (87389)” in the new code.
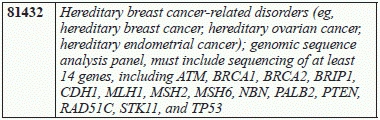
5. Don’t Miss This Genetic Marker Testing
You’ve got a new genetic marker testing code:
“Again, we shall see what payers say about coverage,” Witt says
6. Evaluate This E/M Detail
The following prolonged service codes relate to clinical staff, but CPT® does not define to whom they refer.
Because they state “clinical staff,” they could “refer to an RN but probably not an MA, and it implies that the person who is billing is the clinical staff person which makes no sense. We will have to wait and see what the explanation for this one is at the CPT® meeting in November,” Witt says.
7. VizAblate System Gets a Category III Code
Finally, you have a Category III code to highlight. It is:
0404T Transcervical uterine fibroid(s) ablation with ultrasound guidance, radiofrequency
This code was developed to report the VizAblate System.
What that is: The VizAblate System is a device that is inserted through the cervix into the endometrial cavity, and uses radiofrequency energy to ablate individual fibroids while allowing the physician to see what he/she is doing with intrauterine sonography.
The use of radiofrequency energy to treat fibroids is well established in the literature. “Some physicians where performing this via an open or laparoscopic approach back in the early 1990’s, but without the ability to seeing inside the fibroid at the same time,” Witt says.