Expect 2-Tier Drugs-of-Abuse Reporting for Medicare

The two proposed “G” codes for Medicare drug-test coding are out, and seven different proposed “G” codes are in. That’s the plan currently on the table in CMS’ Clinical Laboratory Fee Schedule (CLFS) preliminary payment determination.
That means when your toxicology lab performs testing for drugs of abuse — both screening and confirmatory testing — you’ll need to learn a new way to report the services in 2016. Read on to get our experts’ guidance on what you need to know beginning January 1.
Alert: This proposal differs from what CMS initially proposed at the July 16, 2015 Annual Clinical Laboratory Public Meeting. That initial proposal was roundly criticized by industry stakeholders such as Lee Hillborn, MD, representing the American Society for Clinical Pathology (ASCP), who commented that “the two-code strategy doesn’t adequately capture” drug testing information.
Follow Medicare Coverage Debate
CMS declined to price the CPT® drug testing codes that were new in 2015. Instead, the agency required your lab to report testing for drugs of abuse in 2015 using two existing HCPCS Level II “G” codes for screening (G0431, Drug screen, qualitative; multiple drug classes by high complexity test method [e.g., immunoassay, enzyme assay], per patient encounter and; G0434, Drug screen, other than chromatographic; any number of drug classes, by CLIA waived test or moderate complexity test, per patient encounter), and 28 new G codes for definitive testing (G6030-G6058). You can soon forget those rules, because CMS has proposed new rules for next year.
The 2016 rules approximate the recommendations represented by several stakeholders at the annual clinical lab meeting, such as JoAnne Glisson, senior vice president of the American Clinical Laboratory Association (ACLA), who recommended “two codes for presumptive testing and four codes for definitive testing,” in an open letter to CMS.
Read on to get the details of the CMS proposal for reporting drugs-of-abuse testing in 2016. You can access the CMS recommendation at www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/ClinicalLabFeeSched/Downloads/CLFS-CY2016-Preliminary-Payment-Determinations.pdf .
Use 3 Codes for Screening in 2016
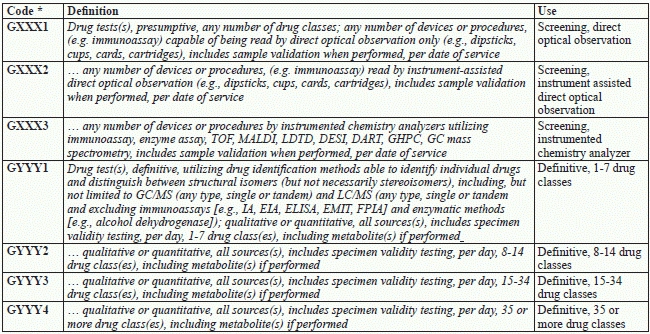
CMS proposes three new codes for presumptive drug screen coding in 2016, as shown in Table 1 (code numbers are not finalized in the CMS preliminary pricing document).
You’ll select the appropriate code based on the lab method used — direct optical observation tests (GXXX1), instrument-assisted direct optical observation tests (GXXX2), or more complex chemistry analyzers tests using methods such as mass spectrometry and gas chromatography (GXXX3).
“Notice that each of these codes is ‘per date of service,’ which means that you’ll report one unit of the appropriate service code for any number of drugs or drug classes, using any number of devices or procedures,” says William Dettwyler, MT AMT, president of Codus Medicus, a laboratory coding consulting firm in Salem, Ore.
Payment plan: CMS has proposed payment for these new codes based on the current value of G0434, with GXXX1 valued at half of G0434, and GXXX2 valued the same as G0434. CMS supports this pricing rationale by stating, “GXXX1 and GXXX2 split the current G0434 into direct optical reading, and instrument assisted optical reading.” Because G0434 is priced to cover the instrument assisted reading, GXXX2 “legitimately represents the work envisioned in G0434” and should be priced the same, while GXXX1 represents only direct reading of cups/dipsticks and should be priced at half of G0434.
Furthermore, CMS recommends pricing GXXX3 at three times G0434 because “The services in G0434 typically can only perform 10-15 tests. The more sophisticated machines in [GXXX3] can perform 2-4 times the number of tests. We believe crosswalking to three times the current code appropriately recognizes the work involved.”
Count Drug Classes to Pick Confirmatory Code in 2016
CMS doesn’t want you to use the CPT® definitive drug codes (80320-80377) when your lab performs a confirmatory drug test following a positive drug screen. Instead, you’ll have four new “tiered” codes to use in 2016, as shown in Table 1.
“Like the presumptive codes, each of these codes has a unit of service, ‘per day,’” Dettwyler advises.
Unlike the presumptive codes, you don’t distinguish these codes based on lab method, but based on the number of drugs or drug classes your lab tests identify. The tiers are one to seven drugs, eight to 14 drugs, 15 to 34 drugs, or more than 35 drugs or drug classes, including metabolites.
Watch validation: All six new G codes indicate that you should not separately bill for validation as part of your drug testing protocol. Validation involves testing to ensure that the specimen is urine, as well as using protocols to ensure that the urine specimen came from the patient. None of these services are separately billable — validation is included in test allowance for drug screens.
Common tests to ensure that the lab has a urine specimen might include urinalysis (81003, Urinalysis, by dip stick or tablet reagent for bilirubin, glucose, hemoglobin, ketones, leukocytes, nitrite, pH, protein, specific gravity, urobilinogen, any number of these constituents; automated, without microscopy) or creatinine (82570, Creatinine; other source) and pH (83986QW — pH; body fluid, not otherwise specified), but you should not separately bill for those services.
Brace for CMS Payment Plan
CMS has proposed payment for these new codes based on the value of 82542 (Column chromatography/mass spectrometry [e.g., GC/MS, or HPLC/MS], non-drug analyte not elsewhere specified; quantitative, single stationary and mobile phase). Based on past stakeholder recommendations for tiered pricing, CMS came up with a plan that values the first two drugs or drug classes at 82542 x 2, and each subsequent drug or drug class at 82542 x 0.10. Because GYYY4 doesn’t have a maximum number, CMS chose 50 drugs or drug classes for pricing (based on commenter recommendations). Here’s what that looks like, based on 2015 CLFS national limit amount payment rates:
Implications: Not everyone is happy with the current CMS proposal. “While I applaud CMS’ attempt to redress the concern of overpayment for drug testing, it has severely missed the mark with its most recent proposal,” says Yussuf Aleem, JD, with Joseph, Aleem & Slowik, LLC in Atlanta. “CMS would have been far better served if it instead adopted revised coverage policies that ensure providers are ordering only medically necessary tests. Based on firsthand experience in the industry, I suspect that a $167 cap on definitive testing will drive a number of labs out of business, particularly those that specialize in drug monitoring the most high-risk patients. This is something we simply cannot afford at a time when more Americans now die from drug overdoses than they do in motor vehicle accidents,” he says.
Table 1: Proposed HCPCS Level II Codes for Drugs-of-Abuse Testing
* Code numbers are not finalized in the CMS preliminary pricing document.