Frequency Is A Factor When Coding Colonoscopies
Are you mystified by the extent of coverage for screening colonoscopies, and what to do when these procedures turn diagnostic or therapeutic midway through the process?
“Many providers are confused about the definition of screening because the codes can vary between average-risk screening and for high-risk screening. If the provider does not make the patient’s risk status clear in the report then mistakes may occur with claims,” says Michael Weinstein, MD, former representative of the AMA’s CPT® Advisory Panel.
Important: As per Medicare, a screening is a procedure done on the patient when he is asymptomatic and there are no symptoms or abnormalities. It is performed to rule out the possibility of a pathology such as cancer.
Read on to take the guesswork out of coding for colonoscopies and bill these claims successfully.
Go By the Risk Profile
According to Medicare, an individual with a strong positive family or personal history of cancer, colorectal cancer, adenomatous polyp, or one who has Crohn’s disease, ulcerative colitis, or Inflammatory Bowel Disease (IBD) is at high risk for developing colorectal cancer, and is a candidate for screening.
In the absence of these factors, the patient comes in under the average risk category. A history of hyperplastic polyps is not included as a risk factor in either case, says Weinstein.
Get Your Codes Right
You need to bill the service differently depending on the severity of the risk factor.
Average risk case: When billing for a screening colonoscopy for an average risk patient, you may use codes:
The ICD-10 codes to use are:
High risk case: When billing for a screening colonoscopy for a high risk patient, use codes:
You have multiple ICD-10 to choose from with high risk cases:
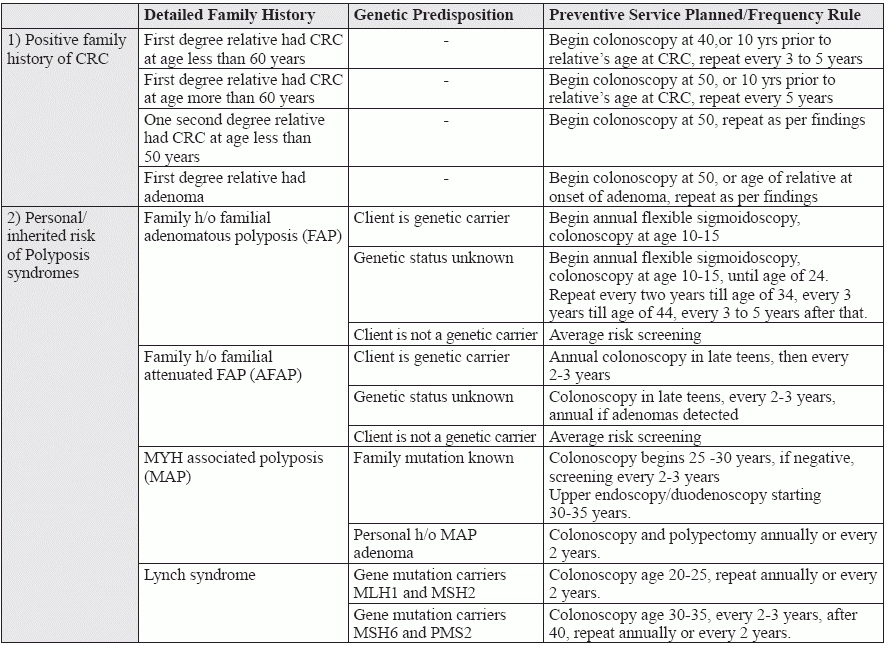
Devise Your Strategy Based On History
If the attending provider decides on the basis of clinical history and findings that the individual is at a high risk, he may go for frequency rules of any one of the following preventive service, as applicable.
Putting it all together: Going by the frequency rules let’s take an example of Mr. X, who meets high risk criteria for colorectal cancer. In this case, you must:
This patient will be allowed coverage for screening colonoscopy as often as once every 24 months. While many private payers accept the G code for colorectal cancer screening, some non-Medicare payers prefer 45378.
Tip: “List a condition that puts the patient at high risk for colorectal cancer as primary diagnosis,” according to the 2016 CPT® coding update by the American Gastroenterological Association (AGA).
How to Get Paid For Associated Services
Anesthesia: To get anesthesia covered for screening colonoscopy, add modifier 33 (preventive service) to the anesthesia CPT® code 00810 (Anesthesia for lower intestinal endoscopic procedures, endoscope introduced distal to duodenum) to imply that the procedure was preventive in nature.
Screening turning therapeutic: In case the provider decides to do a therapeutic intervention during the procedure, add modifier PT (Colorectal cancer screening test; converted to diagnostic test or other procedure), indicating a colorectal cancer screening test which led to a diagnostic procedure to the therapeutic colonoscopy code (4538X) for a Medicare claim; so that only a 20 percent co-pay is payable, and the deductible is waived, says Weinstein. “For non-Medicare claims the modifier is -33.”
Pathology: A procedure begins as a screening colonoscopy, but later on the provider decides to perform a biopsy or polyp removal. In such a case, payment will not be possible under a screening colonoscopy claim, as per Medicare, “and will be subject to deductible and co-pay requirements,” adds Weinstein.
As for commercial payers, some payers may pay for preventive benefits, if you bill the claim with screening as the principal diagnosis and the clinical finding as a secondary diagnosis. Do not forget to add modifier 33, to indicate that intent of the procedure was primarily preventive.
The road ahead: As a general rule, you should look for the private payer’s frequency and diagnosis guidelines, which might differ from Medicare’s, before coding these services. “The United States Preventative Services Task Force recently issued an update for colorectal cancer screening guidelines which may or may not influence private payer’s coverage decisions,” informs Weinstein.