Hone Your Procedure and Dx Coding Skills With This Implant Situation
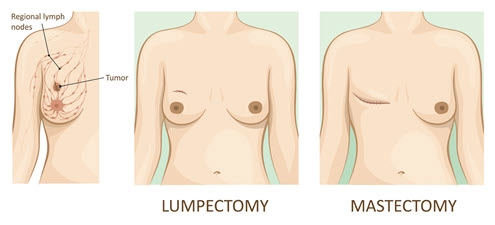
Unit of service can trip you up. Sometimes unusual pathology cases make the best learning tools. Here’s an instance that provides lots of opportunities to illustrate principles for breast procedure coding. And because the case deals with a breast-implant related condition that clinicians are just beginning to define and understand, this case allows you to learn about a new diagnosis code, too. The case: Identify Separate Specimens to Capture Every Code The case involves several distinct specimens that form the basis of your coding. The first specimen is the partial breast resection. You should code the pathologist’s exam of the four blocks of breast tissue and capsule as 88307 (Level V - Surgical pathology, gross and microscopic examination … Breast, mastectomy - partial/simple …). You should additionally report the gross exam to identify the implant as 88300 (Level I - Surgical pathology, gross examination only). The sentinel lymph node is a separate specimen that earns another unit of 88307 (… Sentinel lymph node …) for the pathology exam. The final specimen is the right axillary lymphadenectomy, which you should report as another unit of 88307 (… Lymph nodes, regional resection …). Bundling issues: CPT® also provides 88309 (Level VI - Surgical pathology, gross and microscopic examination … Breast, mastectomy - with regional lymph nodes …) to describe a breast mastectomy specimen that includes lymph nodes. This case doesn’t reflect 88309 because the surgeon identified the breast specimen as a partial mastectomy, and the surgeon separately submitted the axillary lymphadenectomy following an intraoperative consultation. An 88309 specimen includes the entire breast (usually including skin, areola, and nipple), some or all of the axillary lymph nodes, and possibly chest wall muscle. You might see the surgical procedure called radical (or modified radical) mastectomy, complete mastectomy, or total mastectomy. Key: “How you code a breast specimen and lymph nodes depends on how the specimen(s) are identified and submitted,” says R.M. Stainton Jr., MD, president of Doctors’ Anatomic Pathology Services in Jonesboro, Arkansas. You may separately bill an axillary lymph node resection submitted in addition to a distinct breast specimen that is not a complete mastectomy. Sentinel stands apart: You should never bundle a lymph node identified as a sentinel node into another specimen, even if that specimen includes regional lymph nodes (as the complete mastectomy does). The surgeon separately submits a sentinel node identified as the first draining node in the lymph basin. “The pathologist examines a sentinel node with much greater detail involving multiple levels of serial sectioning and staining to identify any hint of the spread of cancer cells,” Stainton says. That service always earns a separate 88307 charge. Count Separate Stains for Full Pay The pathology service for this case includes several special stains that you need to report. For the enhanced cytopathology smear of seroma within the breast implant capsule, the pathologist used a Wright-Giemsa stain to distinguish cell types to help evaluate possible lymphoma. You should code that procedure as 88112 (Cytopathology, selective cellular enhancement technique with interpretation (eg, liquid based slide preparation method), except cervical or vaginal). IHC: The pathologist evaluates two immunohistochemistry (IHC) stains: CD30 and ALK. Although the pathologist documents performing these stains on each of four tissue blocks of the partial mastectomy specimen, you should report just one unit of each stain. Because the unit of service is the partial mastectomy specimen, you should code the two IHC stains as follows: Don’t Miss Intraoperative Service The surgeon requested an intraoperative consultation on the sentinel lymph node specimen in this case, and the pathologist completed a frozen section examination of two blocks from the sentinel node. Based on the pathologist’s reported frozen section results, the surgeon proceeded to perform an axillary lymphadenectomy. You should code the pathologist’s intraoperative consult using the following codes: Dial In Diagnosis Coding Based on the pathologic findings, the final diagnosis for the case is breast implant-associated anaplastic large cell lymphoma (BIA-ALCL). The condition is not breast cancer, but is a type of non-Hodgkin’s lymphoma, which is an immune-system cancer. The cancer cells may be limited to the seroma within the capsule surrounding the breast implant and the capsule itself, but it can spread through the body. ICD-10-CM 2022 added a diagnosis code for the condition — C84.7A (Anaplastic large cell lymphoma, ALK-negative, breast). “The code came with the synonym of breast implant associated anaplastic large cell lymphoma (BIA-ALCL),” notes Amy Pritchett, CCS, CPC-I, CPMA, CDEO, CASCC, CANPC, CRC, CDEC, CMPM, C-AHI, senior consultant at Pinnacle Enterprise Risk Consulting Services LLC in Centennial, Colorado. Guidelines for the code include Use additional code notes that instruct you to use Z98.82 (Breast implant status) or Z98.86 (Personal history of breast implant removal), according to Pritchett. Additionally, ICD-10-CM Official Guidelines added a further guideline, I.C.2.s, specific to BIA-ALCL, which tells you not to “assign a complication code from chapter 19 [Injury, poisoning and certain other consequences of external causes].” In other words, BIA-ALCL is “a type of non-Hodgkin’s lymphoma … found in the scar tissue and fluid near the implant [that] can spread throughout the body” (www.fda.gov/medical-devices/breast-implants/questions-and-answers-about-breast-implant-associated-anaplastic-large-cell-lymphoma-bia-alcl). BIA-ALCL is not a complication of a breast implant after rupturing or malfunctioning. So, you cannot use a code such as T85.79- (Infection and inflammatory reaction due to other internal prosthetic devices, implants and grafts) or T85.43- (Leakage of breast prosthesis and implant) with C84.7A.