Grasp Final CLFS Pricing Details for Your Lab
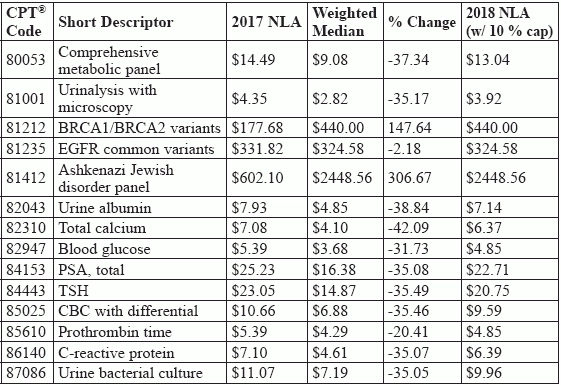
See exceptions to weighted-median valuation. Brace for payment reductions to about three quarters of your lab tests paid under the Clinical Laboratory Fee Schedule (CLFS) in 2018. Overall, the updated fee schedule will account for nearly a 10 percent reduction in the $7 billion that Medicare pays annually for lab tests. How we got here: To comply with the Protecting Access to Medicare Act's (PAMA) mandate to base the lab fee schedule on private payer rates, CMS gathered lab rate and volume data for tests paid on the CLFS and calculated the weighted median for each test. You read about the preliminary payment rates and stakeholder response in Pathology/Lab Coding Alert Vol. 18, No. 12, "Expect Radical Pay Changes for Clinical Lab Tests January 1." Now CMS has issued the final determinations, effective Jan. 1, despite near-universal stakeholder pleas to delay implementation. Let our experts help you unpack what the numbers mean for your lab, and how CMS manages pricing for several "special cases" that aren't subject to the weighted-median formula. Is the New CLFS Representative of All Labs? CMS addressed stakeholder concerns that the gathered data was not representative of the entire lab industry with this statement: "The data reported to CMS captures over 96% of laboratory tests on the CLFS, representing over 96% of Medicare's spending on CLFS tests in Calendar Year 2016. Laboratories from every state, the District of Columbia, and Puerto Rico reported data. This strong response gives us confidence that the final payment rates accurately capture the rates paid by private payors and allow CMS to utilize the power of the private market to help make sure the CLFS pays accurately for tests." But stakeholders, disagreed, such as this statement issued by the American Clinical Laboratory Association (ACLA): "The final payment rates published today make clear CMS ignored Congress's instructions to gather commercial price information from all sectors of the clinical laboratory market and base Medicare payment rates on that data," said ACLA President Julie Khani. Representation: While CMS collected 90 percent of the data from independent laboratories, hospital and physician office labs provide 44 percent of laboratory services to Medicare, according to Debra Rodahl, MBA, MLS(ASCP)CM, ASCLS President, in a statement to CMS. "One unintended consequence of the proposed CLFS is that it may force many laboratories to stop or significantly curtail their testing, particularly rural hospitals, small health clinics, and POLs," stated Michael J. Bennett PhD, FRCPath, FACB, DABCC President, American Association for Clinical Chemistry (AACC), in a letter to CMS. Understand Weighted Mean with Cap CMS collected data on lab test payment rates and volume for 96 percent of the more than 1300 tests on the CLFS. Using the data, CMS calculated the median payment value, with the data weighted to consider the volume of tests paid at each rate. This value becomes the 2018 National Limit Amount (NLA), except for certain circumstances. Phase in: Because of concerns that some tests would see large payment decreases, CMS caps the payment declines at 10 percent per year for calendar years (CY) 2018-2020, and 15 percent per year for CY 2021-2023. Based on the collected data, 58 percent of tests on the CLFS exceeded a 10 percent decline and will have payment reductions phased in over multiple years. The following table shows some of these price changes for representative tests your lab might perform: Watch for Weighted-Median Exceptions In the final determinations, CMS addressed a stakeholder concern that 23 tests that did not have a 2017 NLA value, but that were paid by some local Medicare payers, were not subject to the 10 percent reduction cap. For instance: Code 80061 (Lipid panel) did not have a 2017 NLA amount, but some local payers cover the test, with a median local payment rate of $18.37. The data collected for this code resulted in the weighted median of $11.23, which CMS's preliminary CLFS listed as the 2018 NLA amount. With CMS's final determination correction to use the median local amount in place of the 2017 NLA to determine the 10 percent reduction cap, the new 2018 NLA value for the test is $16.53. With continued annual 10 percent reductions, the 2020 NLA for 80061 would be $13.34 - still above the original $11.23 suggested by CMS. Pap exception: Based on a statutory requirement that sets the Pap test pricing floor at $14.65 for 2018, CMS updated the following codes (short descriptor) to a 2018 NLA of $14.65 from the proposed weighted-median values listed: Similarly, CMS changed the proposed payment for 83037 (Hemoglobin; glycosylated (A1C) by device cleared by FDA for home use) in the final determination. Based on a statutory requirement that the home HbA1C test (83037) garner the same pay as the lab test (83036, Hemoglobin; glycosylated (A1C)), CMS sets the 2018 payment rate for 83037 at the same rate as 83036 ($11.99) instead of the weighted median for 83037, which was $22.50. For codes with no data: CMS does not use the weighted-median formula for pricing the following three groups of codes in the 2018 CLFS and beyond: Instead, CMS uses a different pricing mechanism such as crosswalking or gapfilling. Turn to "Check Out New Code Pricing and More" on page 11 to learn more about these special cases.