Master Pressure Ulcer Culture and Dx Coding
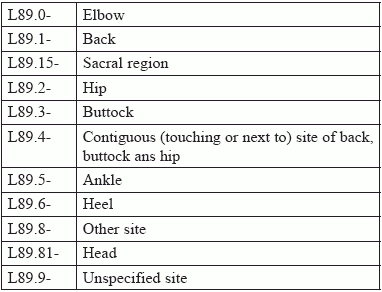
Don’t miss tips on site and stage. When a clinician suspects an infection in a decubitus ulcer, he may send a specimen to your lab to identify any possible infecting organism. Read on for expert tips on how to choose the right CPT® and ICD-10-CM codes for specimens from a pressure ulcer (also called a bedsore or decubitus ulcer). Zero in on Procedure Options To identify the causative microorganism and it’s susceptibility to antibiotics, the clinician may swab the pressure ulcer site. After flushing the ulcer with saline to remove purulent drainage, the clinician typically selects a small area of viable tissue — not eschar or slough — and swabs the area with enough force to produce exudate. For shallow ulcers, the physician would typically order an aerobic culture. For exudate from deeper ulcers, the clinician may request an anaerobic culture, or less frequently, a direct evaluation of the smear. Based on the depth of the swab and the type of test your lab performs, you might report one of the following codes: Capture definitive: If your microbiology lab isolates a colony from either the aerobic or anaerobic culture, the lab analyst may perform additional testing to definitively identify the organism. You should use one of the following codes to bill the definitive testing, based on whether the original culture was aerobic or anaerobic: Don’t miss sensitivity: If the lab goes on to perform sensitivity (susceptibility) testing to determine for antibiotic resistance for the isolate, you should report an additional code to describe that service. CPT® provides multiple codes for susceptibility testing based on lab method, but a common test reports to code 87184 (Susceptibility studies, antimicrobial agent; disk method, per plate (12 or fewer agents)). Conquer Diagnosis Coding With so many pressure-ulcer code choices in ICD-10-CM, choosing the right one can be daunting. We’ve broken it down into four easy steps that will help you select the best code, every time. Step 1: You need to identify the pressure ulcer anatomic site. The ordering clinician should have carefully documented the location of the ulcer, which is the site of the swab specimen. ICD-10 breaks down pressure ulcer sites the following way: Notice that the fourth digit of L89.- indicates the pressure ulcer anatomic site, such as hip or heel. Reporting L89.89- (Pressure ulcer of other site) “means that the provider has indicated where the ulcer is, but there is no specific code under L89.- that specifies the site documented,” says Melanie Witt, RN, CPC, MA, an independent coding expert based in Guadalupita, New Mexico. On the other hand, L89.9- (Pressure ulcer of unspecified site) describes the situation where the ordering physician doesn’t provide more specific information about the site of the ulcer. “Using L89.9- could cause problems for treatment and care reimbursement, because certain care is more appropriate for feet as opposed to the sacrum, hips, or other locations that pressure ulcers may appear,” advises Marcella Bucknam, CPC, CCS-P, COC, CCS, CPC-P, CPC-I, CCC, COBGC, revenue cycle analyst with Klickitat Valley Health in Goldendale, Washington. For instance, whether the treating physician selects oral or IV antibiotics may depend on the ulcer’s location. If the ulcer is on the trunk or sacrum, the treating physician may give oral antibiotics because those areas have good blood flow. But the patient may require IV antibiotics for a pressure ulcer on the lower extremity. Step 2: Identify laterality (left, right, or unspecified) so that you can assign the fifth digit for L89 codes, such as the following: CPT® provides no bilateral pressure ulcer codes, which means that you must separately report right and left codes when pressure ulcers equally affect both sides of regions such as the hips and buttocks. Some sites give even more specific site choices than laterality, such as the following fifth digit options for pressure ulcers of the back: Step 3: ICD-10 categorizes pressure ulcers by degrees of severity, known as stages. The stages correlate to the depth of the tissue damage, and you need that information to assign sixth character of L89 codes. Here’s what the sixth digit means: Clarify: Unstageable is not the same as unspecified. In some cases, the treating physician can’t determine depth or stage of the wound because slough and/or eschar cover the wound bed, often enabling the wound to heal. For that reason, the physician may choose not to remove the covering just to determine the stage, and would designate the pressure ulcer as “unstageable.” On the other hand, “unspecified” means that the medical record gives no indication about the stage of the pressure ulcer. Step 4: Determine if the pressure ulcer involves gangrene. Sometimes infections result in gangrene as conditions in the wound interfere with blood flow and allow tissue death. If the medical record indicates the patient has gangrene, you’ll need to code that first before you dig into the pressure ulcer codes. ICD-10-CM directs you to code the condition with I96 (Gangrene, not elsewhere classified) and sequence it before the specified pressure ulcer.