Know These Differences, Update Your PCM/CCM/Complex CCM Understanding
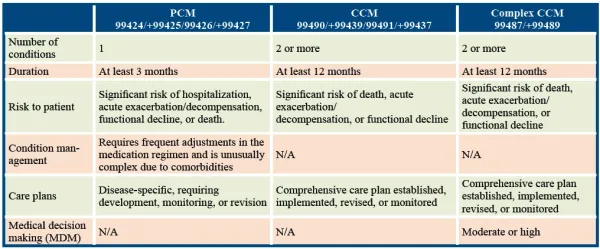
Get ready for the code changes slated for Jan. 1, 2022. Last month, we told you about the addition of principal care management (PCM) codes 99424 (Principal care management services, … first 30 minutes provided personally by a physician or other qualified health care professional, per calendar month), +99425 (… additional 30 minutes …), 99426 (Principal care management services … first 30 minutes of clinical staff time directed by physician or other qualified health care professional, per calendar month), and +99427 (… each additional 30 minutes …) to CPT® 2022. This month, we take a look at the differences between PCM, chronic care management (CCM), and complex CCM to help you get ahead of the care management curve in 2022. Difference 1: Know What Is Meant by “Chronic” Care management services are designed to help manage patients with chronic conditions, which CPT® defines as conditions where “the risk of morbidity without treatment is significant.” Additionally, a condition is “treated as chronic whether or not stage or severity changes.” In other words, a condition is chronic no matter what its severity or whether it is stable, in a state of exacerbation, or in a stage of progression. As for duration, CPT® guidelines describe a stable, chronic illness as one that has “an expected duration of at least one year or until the death of a patient.” However, the care management service codes provide different definitions for the duration of the condition that may influence code choice depending on the circumstances. Difference 2: Know the Eligibility Requirements The eligibility criteria for the care management codes are fully laid out in the code descriptors for 99242/+99427, 99490/+99439/99491/+99437 (Chronic care management services …), and 99487/+99489 (Complex chronic care management services …). Aside from documenting the above, you will need to document the following: Comprehensive care plan: To code CCM and complex CCM, you will need to show your pediatrician “established, implemented, revised, or monitored” a comprehensive care plan. Per CPT® guidelines, this should be “based on a physical, mental, cognitive, social, functional, and environmental evaluation,” and should include, but not be limited to, the following: MDM: Complex CCM requires a record of your pediatrician engaging in moderate- or high-level medical decision making (MDM) as determined by the office or other outpatient services MDM table. Neither PCM nor CCM has this requirement. Difference 3: Know Who Can Provide the Service Both clinical staff under the direction of a physician or other qualified healthcare professional (QHP) and physicians or other QHPs themselves can provide PCM and CCM. Only complex CCM cannot be provided by clinical staff under the physician’s or QHP’s direction; it can only be provided by a physician or other QHP. Remember: QHPs include physician assistants (PAs), certified registered nurse practitioners (CRNPs), or clinical nurse specialists (CNS), while clinical staff include medical assistants, licensed practical nurses (LPNs), registered nurses (RNs), and others depending on the scope of practice as defined by state law. Difference 4: Know How to Count Time for the Service Counting time for care management services can be tricky because time parameters change for some services and provider type, as the following table shows: Why? Complex CCM patient care is more time-consuming than PCM or CCM because care has to involve moderate- or high-level MDM and the patient has to receive “three or more therapeutic interventions such as medications, nutritional support, or respiratory therapy,” per CPT® guidelines. So, the time threshold for 99487 rises to “60 minutes of clinical staff time directed by a physician or other qualified healthcare professional, per calendar month, while the add-on code, +99489, allows you to document an additional 30 minutes of clinical staff time,” notes Kent Moore, senior strategist for physician payment at the American Academy of Family Physicians. And don’t forget: “Some practices do not even document care management time, so the codes cannot even be used,” says Marcella Bucknam, CPC, CCS-P, COC, CCS, CPC-P, CPC-I, CCC, COBGC, revenue cycle analyst with Klickitat Valley Health in Goldendale, Washington. To remedy this, Bucknam suggests coders “create a process to track it or create a special build in your electronic medical record (EMR) to track and calculate minutes spent providing the service.”