
Use This Guide to Find Physeal Fracture Codes Fast

And know with, without manipulation to find the right procedure. Salter-Harris fractures are among the most common injuries found in pediatric medicine, accounting for up to 30 percent of children's bone injuries. As they occur in the growth plate, or physis, of the long bones, they are conditions unique to childhood. The bad news? If left untreated, they can cause problems as the bone grows. The good news? The most common physeal fractures heal easily without surgery, usually by the pediatrician performing manipulation, or closed reduction, on the bone and putting the bone in a sling, splint, or cast to keep it immobile while it heals (Source: https://www.healthline.com/health/salter-harris-fracture). The even better news for coders? The fractures and the procedures that correspond with them are not hard to document if you follow this advice. Know the Bone, Find the Code Because the S00-S99 codes in ICD-10 are arranged by anatomical region, Salter-Harris fracture codes can be found in a number of different blocks: Know the Break, Get Specific Each code block is then broken down into fracture types. Ruby O'Brochta-Woodward, BSN, CPC, CPMA, CPB, COSC, CSFAC, AAPC, coding and compliance manager at Suburban Imaging in Minneapolis, Minnesota, notes that although the Salter-Harris classification identifies numerous types of physeal fractures, ICD-10 only provides codes for types I though IV (except S89.2 and S89.3, which only have codes for types I and II). In the pediatric setting, Donelle Holle, RN, President of Peds Coding Inc., and a healthcare, coding, and reimbursement consultant in Fort Wayne, Indiana, reminds coders, you will probably only see the first two types. This is partly because "a type I is often diagnosed strictly by mechanism of injury and exam," according to O'Brochta-Woodward, "and is often not visualized on x-ray." For other kinds of physeal fractures, there are codes for both unspecified and "other." "Unspecified," according to O'Brochta-Woodward, "would, like any of the unspecified codes, be used if the provider simply documents that it is a physeal fracture but doesn't give us the type." The "other" codes, O'Brochta-Woodward goes on, "would be for those fractures documented but for which there is no code. For example, O'Brochta-Woodward explains, "if the patient presented with a crushing injury involving the physis, this would be a type V and would have to be coded as 'other.'" Fun fact: O'Brochta-Woodward notes that you can remember the first five Salter-Harris classifications using the mnemonic SALTR: Type 1: Slip/Separated/Straight across (fracture of the physis (growth plate) cartilage) "As coders, however," says O'Brochta-Woodward, voicing a note of caution, "we can't assign the type - the provider must document it." Know Upper, Lower, Laterality, Encounter Type for Precise Coding Fortunately for coders, ICD-10 then breaks down the codes very specifically, with precise fifth digits for the upper and lower portions of the larger bones, sixth digits for laterality in the case of all bones, and a seventh digit detailing the encounter and complications that may arise: So, the initial encounter for a Type 1 Salter-Harris fracture of the upper end of the right tibia would be coded as S89.011A. Know What Was Done "CPT® coding," O'Brochta-Woodward tells coders, "would be based upon where the fracture is, and which type it is. Salter I fractures," O'Brochta-Woodward goes on to point out, "would be nonmanipulative fracture management." So, for example, O'Brochta-Woodward notes, a Salter-Harris I of a distal femur S79.11- would generally be 27516 (Closed treatment of distal femoral epiphyseal separation; without manipulation). Similarly, Holle points, coders would document "treatments for fractures seen in children due to injuries like falls" with such codes as "These fractures," Holle notes, "could be taken care of by pediatricians by using simple splints or even buddy taping as they do not require manipulation." Type II fractures," O'Brochta-Woodward explains, are treated differently and "need to have a reduction done. If the pediatric practice does fracture reductions," O'Brochta-Woodward goes on, "then coders would use a code such as 27517 (Closed treatment of distal femoral epiphyseal separation; with manipulation, with or without skin or skeletal traction) for a type II fracture of the distal femur." Billing note. Holle points out that these procedures have "a global period of 90 days, so if the child is rechecked for the fracture, that visit has already been reimbursed and there would be no charge." However, Holle adds, "you can charge for changing the splint if one is used."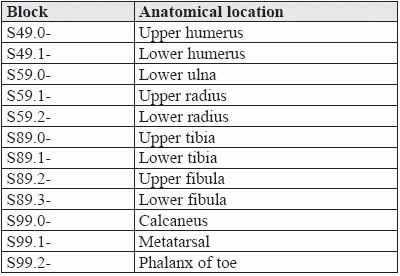
Type II: Above/Away (fracture above the physis and in the metaphysis or away from the joint)
Type III: Lower (fracture below the physis and in the epiphysis, or toward the joint or rounded part of the bone)
Type IV: Through everything (fracture through the metaphysis, physis, and epiphysis)
Type V: Rammed (the physis is crushed).



