Expect a High Focus on Value from CMS in 2015

Agency proposes PQRS changes and more in proposed MPFS.
The proposed Medicare Physician Fee Schedule is hot off the press with both expected and unexpected changes. Therapy cap exceptions and Medicare payment rates would stay the same until March 31, 2015, thanks to the Protecting Access to Medicare Act (PAMA) of 2014.
No surprise: Without Congressional action, therapy caps go back into full effect, and Medicare payments are looking at a 20.9 percent cut starting April 1, 2015.
Look Out: Impending CPT® Revaluing
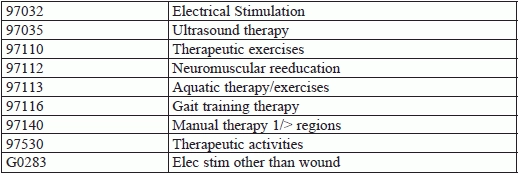
CMS is under mandate to review how certain high-expenditure CPT® codes are valued. In response, the proposed MPFS has listed specific CPT® codes up for review and is suggesting a new process for determining payment rates.
“This list includes the following CPT® codes reported by physical therapists,” notes Gayle Lee, JD, director of federal payment policy and advocacy for the American Physical Therapy Association.
Watch for New Value-Based Modifier
CMS announced routine updates for PQRS, including an increase to nine required reportable measures. But the agency is looking to do even more with quality reporting.
“One of the most significant proposals in the rule relates to the application of the value-based modifier (VM) to non-physicians, including physical therapists, in 2017, that are in groups of two or more solo practitioners,” Lee points out.
CMS’ intent is to promote better care, but experts are concerned whether adding the VM will actually accomplish this.
The VM “is related to PQRS participation as the effect of how your value scores in relation to others affects your payment under the MPFS,” explains Christina Metzler, chief public affairs officer for the American Occupational Therapy Association.
AOTA is analyzing how this change would affect private practices.
Of note: CMS made no update to the G-code reporting. “AOTA will be submitting comments, however, suggesting that this program needs to be carefully examined,” Metzler says. Although the association believes G-code reporting has potential, “AOTA is not convinced that the G-Code reporting for therapy as it stands will generate good, useable data on which to make policy changes.”