Don't Miss These Final 5 HCPCS Code Changes

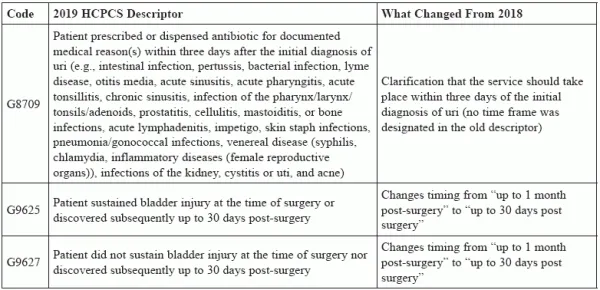
Pay special attention to the revision of G9633. Just because code changes for each upcoming year are released in the fall doesn’t mean adjustments can’t be made later. That happened with some HCPCS codes urologists might report, so be sure you’re up-to-date on the current descriptors. Real world application: “These HCPCS diagnostic codes have rarely been used by urologists in the past, but are available to clarify a clinical scenario,” says Michael A. Ferragamo, MD, FACS, clinical assistant professor of urology at the State University of New York at Stony Brook. “While these are HCPCS codes, they are not billing codes per se but documentation codes, used for MIPS #065 (G8709),” explains Jonathan Rubenstein, MD, compliance officer and medical director of coding and reimbursement for Chesapeake Urology in Towson, Md. The codes related to two quality measures: “The codes were created to help physicians appropriately document these measures,” Rubenstein says. Example 1: Quality measure #434 is used to document the percentage of patients undergoing pelvic organ prolapse repairs who sustain an injury to the ureter recognized either during or within 30 days after surgery. Instructions explain that “this measure is to be submitted each time an anterior and apical prolapse repair surgery is performed during the performance period ending November 30. There is no diagnosis associated with this measure. This measure may be submitted by Merit-based Incentive Payment System (MIPS) eligible clinicians who perform the quality actions described in the measure based on the services provided and the measure-specific denominator coding.” Example 2: Code G9631 is reported if a patient sustains an injury at the time of the procedure or if the injury is discovered less than 30 days post-surgery, unless there is an exception (G9632: medical reasons for not reporting ureter injury (e.g. gynecologic or other pelvic malignancy) documented, concurrent surgery involving bladder pathology, injury that occurs during a urinary incontinence procedure, patient death from non-medical causes not related to surgery, patient died during procedure without evidence of ureter injury). The measure it not met (good) if the patient did not sustain ureter injury at the time of surgery nor discovered subsequently up to 30 days post-surgery (G9633). .... “As you can see,” Rubenstein adds, “the old G9633 is now the new G9632.” 30 day question: Why make such a small change to a descriptor as changing the time frame from “up to 1 month” to “up to 30 days”? “It’s to to reduce ambiguity,” Rubenstein says. “Some months are 30 days, some are 31, and one is sometimes 28. So which is it? That is what physicians may ask, so specifying the number of days helps clarify what the code represents.”