2018 RAI Manual: Note These Important Changes
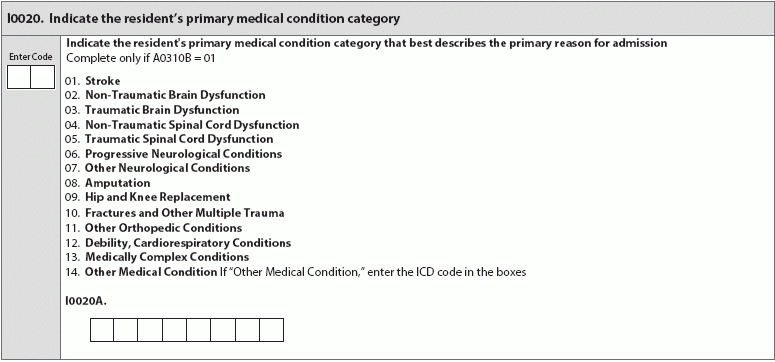
This year’s RAI Manual arrived a few weeks early — dive in now so you’re adequately prepared when it becomes effective this October. The long-anticipated Long-Term Care Facility Resident Assessment Instrument 3.0 User’s Manual Version 1.16 is finally here, leaving you just over a month to familiarize yourself with the changes before the accompanying version of the MDS goes into effect on Oct. 1. With 514 replacement pages — and the shadow of the Patient-Driven Payment Model (PDPM) lurking in one corner of everyone’s minds — the latest RAI Manual interpretations and guidance may have you worried about how you can best deliver and document care. “As has been true with the many challenges faced by LTC facility staff, each member of the interdisciplinary team (IDT) must take responsibility and learn the intent, changes, and clarifications for each section he/she will be signing their name in Z0400 attesting to complete accuracy. It is a huge responsibility and the fact that manual was released earlier than projected, we can find the silver lining in that cloud — we have more time. Each member of the IDT now should have their copy of their section and reviewing it carefully, asking questions, and being attuned and attentive to any training possible. Another part of the good news is that the changes are printed in the color red making it much easier to see those changes and clarifications. Thank you, CMS!,” says Jane Belt, MS, RN, RAC-MT, QCP, curriculum development specialist at American Association of Nurse Assessment Coordination (AANAC) in Denver. The Centers for Medicare and Medicaid (CMS) promises that training, including first-come, first-served webinars, will be available to help the long-term care industry acclimate to new regulations, requirements, and guidance. Resource: Keep an eye on CMS’s YouTube channel for training videos pertaining to the MDS and RAI Process. You can access the videos here: www.youtube.com/user/CMSHHSgov. Look for Adjustments in Language More inclusive language, especially concerning communication, immediately jumps out as a major change in the RAI Manual’s guidance. As an example, look for Item B0700 (Makes Self Understood). This version of the RAI Manual adds instructions for assessment that seem like common sense but may give some people pause: “Assess using the resident’s preferred language or method of communication” (emphasis added to reflect addition). Though this addition first appears in B0700 (Makes Self Understood), the adjustment is made to assessment instructions throughout the manual. “As a part of this added instruction was the common theme for interview is that ‘resident interview items are not directly dependent upon one another, inconsistencies in coding among these items should be evaluated.’ Who will be doing that evaluation? Surveyors for one! If there are any resident interview items that were coded on the MDS, all interviews will need to show that the interview was conducted. Another very clear instruction for interviews was that if the resident interview was not completed in the observation period in a timely manner, the Staff Assessment should not be coded,” Belt says. The manual adds sign language as an alternative method of communication in assessment, but doesn’t offer any guidance on conducting the assessment with a staff member proficient in American Sign Language. See story on page 102 in pdf for more information on facilities’ responsibilities for ensuring effective communication with residents, including sign language interpretation. Evaluate Specific Section GG Changes This version of the RAI Manual encourages the nurse assessment coordinator (NAC) or whoever is filling out the MDS to really search for additional context when conducting assessments. For various items in Section GG (Functional Abilities and Goals), the RAI Manual urges NACs to look to residents’ families or representatives and bring them — and their knowledge — into the conversation. The additional context can go a long way in helping NACs establish goals that all pertinent parties find realistic and manageable, while still putting residents’ wishes first. The new RAI Manual also helps NACs better understand some terms that were previously vague. For example, “Qualified Clinician” is now defined: “Healthcare professionals practicing within their scope of practice and consistent with Federal, State, and local law and regulations” (page GG-9). Note: In item GG0130 (Self Care 3-day assessment period Admission/Discharge), the RAI Manual explicitly notes, in an addition, that CMS “anticipates that an interdisciplinary team of qualified clinicians is involved in assessing the resident during the three-day assessment period” — so make sure your team is in place and that the care they provide is documented. (See page GG-9.) Also look for increased clarification and new ever-helpful coding scenarios. Section I Takes on New Prominence CMS is gearing up to truly patient-centered care, and the change is reflected in the increasing significance of Section I (Active Diagnoses). Look for two new items on the final version of the MDS, also effective Oct. 1, 2018: I0020 and I0020A (Indicate the Resident’s Primary Medical Condition Category). The RAI Manual notes on page I-1 CMS’s rationale for these new items, noting that there’s now a place to record the de facto medical reason a resident ends up in a nursing facility, saying, “Disease processes can have a significant adverse effect on residents’ functional improvement.” “This Primary medical condition category is only completed on the PPS 5-day assessment. The reason? It is used as a risk adjustor for the SNF Quality Reporting Program (SNF QRP) functional outcome measures and that data collection period begins Oct. 1, 2018. As this data is collected the results will be used to determine if the facility will experience a 2 percent reduction in the annual payment update as of Oct. 1, 2019,” Belt says. Item I0200 (Indicate the Resident’s Primary Medical Condition Category) “identifies the primary medical condition category that resulted in the resident’s admission to the facility and that influences the resident’s functional outcomes,” the RAI Manual says. If the resident’s primary medical condition is not listed in any of the coding choices for I0200, Code 14, (Other Medical Condition), and then look to I0200A, where you’ll need to include the “International Classification of Diseases (ICD) code, including the decimal.” Note: Filling out I0200A with an ICD-10 code is appropriate only if the resident’s primary medical condition is not listed. If the primary medical condition is listed in coding choices 1-13, skip I0200A. Beware: ICD-10 accuracy will become a major determinant in evaluating whether residents are receiving appropriate care — and therefore whether facilities receive appropriate reimbursement. See story on page 97 for more information on the increasing significance of Section I (Active Diagnoses) and ICD-10 fluency. Section M Again Refined Pressure ulcers/injuries continue to remain a problem for residents in nursing facilities, and with each new version of the MDS and RAI Manual, CMS continues to refine the language and guidance surrounding their assessment, care, and coding. The biggest changes in this year’s versions of the MDS and RAI Manual are the updated incorporation of the actual language pressure injury specialists from the National Pressure Ulcer Advisory Panel (NPUAP) use to describe, assess, and evaluate the wounds. Look for the next issue of MDS Alert for more in-depth guidance and expert tips on best practices you’ll need to adjust for both pressure injury care and coding. Renewed Focus on Drug Regimen Review (DRR) in Section N Though the current Long-Term Care Survey Process (LTCSP) regulations require a pharmacist to review each resident’s drug regimen monthly (see story “Item Focus: Understand Drug Regimen Review Expansions” in MDS Alert Volume 16, Number 8 for more information), the similarly named addition to Section N is wholly separate, though the requirements may sound familiar. Again, the change reflects CMS’s moves toward patient-centered care, with checks and balances to make sure that the care delivered by a facility is the care clinically required by each individual resident. Subsequently, it’s no surprise that a drug regimen review must be completed upon each resident’s admission — and documented in the MDS. The MDS 5-day Prospective Payment System (PPS) assessments now feature item N2001 (Drug Regimen Review) along with item N2003 (Medication Follow-Up), which is applicable only when the drug regimen review reflects issues or inconsistencies. The RAI Manual lists conditions that could qualify as issues in N2001 (Drug Regimen Review) on page N-16: “Clinically significant medication issues may include, but are not limited to: Item N2003 (Medication Follow-Up) allows for the MDS coder to reflect that any issues were resolved with the appropriate steps to ensure each resident’s safety and health — and clinically appropriate medication. Reference Information Included, Too Don’t forget that your state or region may have made personnel changes for your State RAI Coordinator or RAI Panel Member. You can access the current representatives and their contact information in the updated RAI Manual Appendix B, here: https://downloads.cms.gov/files/Appendix-B-07-26-2018.pdf.