Fibroid Coding Got You Frustrated? 5 Myth Busters Fix Your Claims
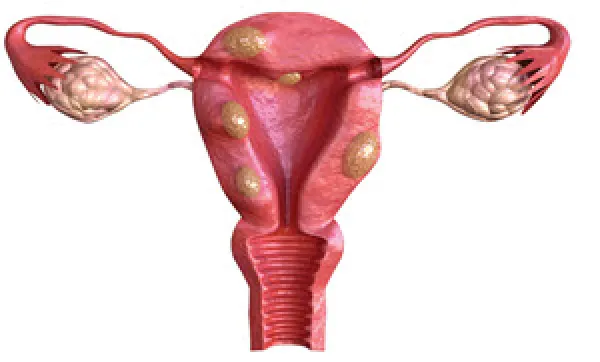
Find out what your fibroid diagnosis options are. If you’re reporting uterine fibroid removal, you need to know two things: Simplify this complicated coding scenario by busting the following five myths. You’ll know where to look in both your ICD and CPT® manuals before the fibroid report lands on your desk. Don’t Confuse Fibroids With Polyps Myth: Fibroids and polyps are essentially the same thing. Reality: True, fibroids and polyps are both growths, but one occurs in the endometrial lining while the other occurs in the muscle. Polyps are small growths on the surface of the uterine wall that are easy for the ob-gyn to remove. In other words, they are an overgrowth of the endometrial lining. They are intracavitary lesions, experts say. Fibroids (or myomas) are larger and are usually imbedded in the smooth muscle of the uterine wall. They are almost always benign, but in rare circumstances, they can become a sarcoma (muscle cancer). These growths require more work to remove, hence the procedures associated with fibroids tend to have more relative value units (RVUs). They occur in three main locations: If the physician does not specify the location of the uterine fibroid, assign D25.9 (Leiomyoma of uterus, unspecified) as the diagnosis. Important: You should report these fibroid codes based on size, location (the 4th character), and number. Sometimes, ob-gyns may have trouble distinguishing between a small fibroid and a large polyp, but they do have different appearances and textures when visualized during the procedure. If you don’t have enough information to choose your ICD-10 code, you may need to wait for the pathology to return for a final diagnosis (a delay of 10 days or so). Examine Your Hysterectomy Options Myth: If your ob-gyn removes a fibroid and the uterus entirely, then you should report both procedures. Reality: You would not code the fibroid removal separately if the ob-gyn is removing the uterus. In other words, if the ob-gyn removes the uterus entirely, they performed a hysterectomy. In the process, they removed the accompanying fibroids attached to or inside the uterus. Hysterectomy is the most common surgical treatment option, but only when the fibroids are causing problems, such as abdominal pain or heavy bleeding. Without removal of the uterus, recurrence of fibroids is common. The code assignment will depend on the type and extent of the hysterectomy, says Melanie Witt, RN, MA, an independent coding consultant in Guadalupita, New Mexico. Example: Because the patient is older than 50 and has multiple fibroids, your ob-gyn performs a total abdominal hysterectomy (58150, Total abdominal hysterectomy [corpus and cervix], with or without removal of tube[s], with or without removal of ovary[s]). You would not report an additional code for the fibroid removal. Hem in Your Hysteroscopy Choices Myth: Your ob-gyn won’t treat fibroids via a hysteroscopy. Reality: An ob-gyn may treat a patient with fibroids with a hysteroscopy. Hysteroscopic submucous resection removes a portion of the protruding fibroid and preserves fertility. The hysteroscopic procedure requires the close monitoring of distention media and electrosurgical devices, as well as a patient’s anatomy, to avoid perforating the uterus. Ob-gyns usually perform this straightforward approach for intracavitary (submucosal) fibroids. Example: Your ob-gyn removed polyps and fibroids by hysteroscope. The pathology diagnosis is fibroid. You should report 58561 (Hysteroscopy, surgical; with removal of leiomyomata). Note that if the ob-gyn also performed a dilation and curettage (D&C), you cannot bill both 58561 and 58558 (Hysteroscopy, surgical; with sampling [biopsy] of endometrium and/or polypectomy, with or without D&C), as these codes are permanently bundled and no modifier is allowed to bypass the edit. Master Myomectomy Codes Myth: A myomectomy means the ob-gyn takes more than just the uterine fibroids. Reality: Actually, an open myomectomy (58140-58146) or laparoscopic myomectomy (58545-58546) means the ob-gyn removes the uterine fibroids only, which preserves fertility. Example: The ob-gyn sees a 32-year-old patient who has never had a child but would like to. She complains of heavy menses with anemia. On examination, the physician finds a 15-week uterus with multiple fibroids that distort the endometrium. Because the patient wishes to have children, she elects to have a myomectomy, which the ob-gyn performs using an abdominal approach. The pathology report shows six intramural myomas. For this case, you should report 58146 (Myomectomy, excision of fibroid tumor[s] of uterus, 5 or more intramural myomas and/or intramural myomas with total weight greater than 250 grams, abdominal approach) with D25.1. Make Use of Embolization or Ablation Options Myth: Your ob-gyn can treat uterine fibroids only with a hysterectomy, hysteroscopy, or myomectomy. Reality: You may see the ob-gyn use other methods when treating uterine fibroids. CPT® now has codes for uterine fibroid ablation and uterine fibroid embolization procedures. An ablation procedure destroys fibroid tissue by inserting special instruments into the cervix or via a laparoscope to target the fibroids with extreme heat or cold, electrical current, radiofrequency, or lasers. These methods soften, weaken, break up, or shrink fibroids to eliminate symptoms. Uterine fibroid embolization, on the other hand, shrinks the fibroids by cutting off the blood supply. Your code choices are as follows: