Pinpoint Differences for TM Repair Coding Success
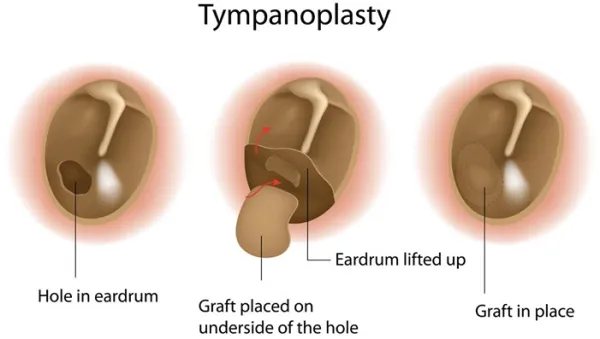
Dig deep into descriptors to better understand these services. Most otolaryngology coders, beginner or advanced, will attest to struggling to understand some of the fundamental differences between the various tympanic membrane (TM) repairs at some point in their careers. While the underlying procedures are similar, there are a few key points you can identify to easily discern between them. Read on for our top advice on acing these claims. Think TM Repair for Patches, Myringoplasty for Grafts It’s easy to fall for the assumption that myringoplasties and TM repair procedures are one and the same. Even though they share several overlapping features, there are a few variables at play that will determine which of the following CPT® codes to report: First, let’s analyze the fundamental characteristics of codes 69610 and 69620. To begin, the surgeon is performing both for the same underlying reason — “to repair the tympanic membrane,” says Ronda Tews, CPC, CHC, CCS-P, AAPC Fellow, director of billing and coding compliance at Modernizing Medicine in Boca Raton, Florida. The TM defect can be deliberately created, for example, to facilitate putting a pressure-equalizing (PE) tube in the eardrum, or it can be traumatic. Regardless of the etiology, the means by which the ENT repairs the perforation will determine how you code a given surgical report. The difference: The extent of work involved in each code is what sets the two apart. For the simplest of repairs, use 69610. “In addition to the steps included in 69610, 69620 also includes dissolvable packing and a fat graft plug or a piece of fascia being placed medial to the eardrum over the packing. A tympanomeatal flap may be raised, and any incisions are sutured a dressing is applied. You should also note that, when performed, the harvesting of a donor graft is included in the code and not reported separately,” explains Tews. Bottom line: Code 69610 represents a less extensive procedure, and you’ll typically see documentation of either a paper patch or Gelfoam® used to repair the perforation. The work of 69620 is more complex and involves harvesting a separate graft to surgically repair the eardrum. “The grafting material used includes a piece of fascia or a plug of fat,” and because the descriptor for 69620 indicates “surgery confined to the drumhead and donor area,” the myringoplasty repair includes the graft, explains Barbara J. Cobuzzi, MBA, CPC, COC, CPCO, CPC-P, CPC-I, CENTC, CMCS, of CRN Healthcare Solutions in Tinton Falls, New Jersey. Tip: Both 69610 and 69620 represent unilateral procedures. For TM repair in both ears during the same session, be sure to append modifier 50 (Bilateral procedure) or -LT (Left side) and -RT (Right side), depending on payer preference. Confirm Middle Ear Entry, Inspection Before Coding Tympanoplasty During tympanoplasty, the surgeon repairs a hole in the patient’s eardrum and reflects the TM forward to inspect the auditory ossicles and remove any adhesions, skin debris, or cholesteatoma in the middle ear. If needed, the ENT reconstructs the ear canal, makes an incision into the tympanic attic, and/or repairs the small bones of the middle ear — malleus, incus, and stapes — before harvesting a fascial graft or other tissue to repair the tear in the eardrum. Key: To report a tympanoplasty code for the repair, the middle ear must be entered and inspected. The documentation should indicate the ENT examined and touched the ossicles. The three CPT® codes for tympanoplasty are distinguished by whether the physician only reconstructs the eardrum to repair a perforation or also completes other repairs: These procedures do not include the removal of the mastoid (mastoidectomy), so the distinctions lie in what is done to the ossicular chain — the three bones in the middle ear that are necessary for hearing. The difference: During 69631, the ENT only repairs the hole in the eardrum. Code 69632 represents eardrum repair plus ossicular chain reconstruction — i.e., sculpting or repositioning of the middle ear bones. In 69633, the most extensive of the three procedures, the surgeon repairs the eardrum and reconstructs the ossicular chain using a synthetic prosthesis to replace bones that aren’t working correctly. Don’t Forget These 3 Tympanoplasty Coding Tips 1. Indicate laterality: As with the first set of repair codes, the tympanoplasty codes are unilateral. Include modifier 50 or -LT and -RT when billing a bilateral procedure. 2. Ignore the approach: Your otolaryngologist might choose to complete tympanoplasty by using either a transcanal approach (through the ear canal) or a post-auricular approach (by making an incision behind the ear). The approach will not affect your code choice; only the procedure itself will dictate how you file. 3. Separately report a graft: “Unlike 69620, codes 69631-69633 do not refer to the donor harvest if a graft is used,” Cobuzzi notes. “The harvest of the graft is separately reportable when the otolaryngologist obtains cartilage, fascia, or other tissue through a separate incision. It is paramount that the separate incision (usually from the opposite side) be documented in the operative note in order to bill the graft with the appropriate code. However, the separate incision need not be on the opposite side to be codable. It just needs to be clear in the documentation that the graft was harvested from a separate incision.”