Big Changes Coming Via Proposed Resident Classification System
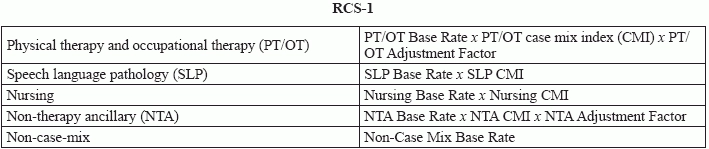
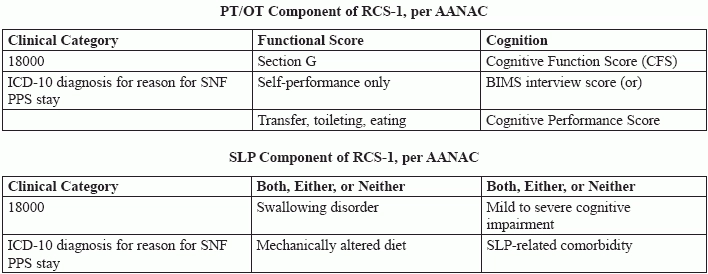
The proposed rule categorizes therapy and payment completely differently than RUG. Back in may 2017, CMS released the advanced notice of proposed rule making. In that document, the resident classification system (RCS) version 1 was proposed to replace RUG 4 system for Medicare reimbursement in skilled nursing facilities, says Jessie McGill Rn, RaC-Mt, curriculum development specialist at the American association of nurse assessment Coordination (AANAC) in Denver in a recent webinar about upcoming changes to the MDS. The RCS-1 system is much different than the currently employed RUG system. "There are two key reforms to improve payment accuracy and strengthen incentives to provide the appropriate level and quality of care," says Kris Mastrangelo, president and CEO of Harmony Health International in Topsfield, Massachusetts, in a recent webinar: There are five main components to the RCS-1 system of payment, which will be divided into four major cost categories, like this, according to AANAC: Each of these components are further divided into groups: PT/OT has 30 groups, SLP services has 18 groups, nursing services has 43 groups, and non-therapy ancillary has six groups. If you're don't currently use ICD-10 very frequently, RCS-1's reliance on MDS item I8000 (Additional Active Diagnoses) will bolster your familiarity, as both the physical therapy and occupational therapy category and the speech language pathology category rely on it for scoring and determining classification into groups. Both of these therapy component formulas depend on MDS items. The PT/OT component relies on item information from Section C (Cognitive Patterns), Section G (Functional Status), and Section I (Active Diagnoses). The SLP component relies on item information from Section C (Cognitive Patterns), Section I (Active Diagnoses), and Section K (Swallowing/Nutritional Status). The nursing and non-therapy ancillary components also depend on information coded across basically the entire MDS. Unsurprisingly, because they take into account so many other diagnoses, treatments, and statuses, the nursing and non-therapy ancillary components are more reliant on the groupings and don't have quite as simple formulas. You can find a worksheet for RCS-1 from CMS here: https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/SNFPPS/Downloads/RCS_I_Logic-508_Final.pdf. So far, there's no indication of the timing of the transition to RCS-1, but all signs are pointing toward "when" and not "if." The technical specifications make no mention of RCS-1 going into effect Oct. 1, 2018, McGill says, and therefore RUG levels should stay the same for now, including a lack of change to Section Z (Assessment Administration).