
Coding Step-By-Step: Break Down The New Item C1310
Mistake: Don’t rely on coma or stupor diagnosis to code C1310D.
You’ve probably started coding the new item C1310 — Signs and Symptoms of Delirium (from CAM ©), but are you coding it correctly? If you’re relying on your old delirium coding know-how, you could be making some basic (but costly) mistakes. Here’s what you need to know to code this new item.
Follow 4 Steps to Assess C1310 Items
As of Oct. 1, 2016, item C1310 replaced the old items C1300 — Signs and Symptoms of Delirium and C1600 — Acute Onset of Mental Status Change. You’ll notice some of the same sub-items in C1310, such as inattention, disorganized thinking, and altered level of consciousness. But the latest version of the RAI Manual nixed the sub-item for psychomotor retardation and included the acute onset of mental status change sub-item, which used to be the separate item C1600.
The Centers for Medicare & Medicaid services (CMS) adapted the sub-items in C1310 from the Confusion Assessment Method (CAM©), notes Carol serici Griffin, Rn, Bs, onC, RaC-Ct, State of Ohio RAI Coordinator. You should code C1310 after completing the Brief Interview for Mental Status (BIMS) or staff assessment.
The RAI Manual provides you with the following four steps to assess the items in C1310:
1. observe resident behavior during the BIMS items (C0200 – C0400) for the signs and symptoms of delirium. Increasing the frequency of assessment (as often as daily for new admissions) may improve the level of detection.
2. ask staff members about their observations of delirium signs and symptoms if the Staff Assessment for Mental Status items (C0700 – C1000) was completed instead of the BIMS.
3. Review medical record documentation during the seven-day look-back period to determine the resident’s baseline status, behaviors that might’ve occurred, and fluctuations in behaviors. The medical record may show you behaviors during the look-back period that you did not observe during the BIMS.
4. interview staff, family members and others who were in a position to observe the resident’s behavior during the seven-day look-back period.
Pay Attention to Coding Instructions for C1310A
Interviewing the resident’s family or significant others is especially important when you’re coding sub-item C1310A — Acute Onset Mental Status Change. You should also carefully review the resident’s medical record prior to the seven-day look-back period to determine the resident’s usual mental status, the RAI Manual instructs.
For C1310A, you’re looking for a noticeable change in the resident’s mental status. This could involve a resident who is usually noisy or belligerent becoming quiet, lethargic or inattentive. Or, a resident who is usually quiet and content suddenly becomes noisy and restless. This will even include a resident who is normally able to find his way around the unit but begins to get lost easily.
Example: The resident was admitted to your nursing home four days ago. Her family reports that she was alert and oriented prior to admission. During the BIMS, however, she is lethargic and incoherent.
How to code: You would code item C1310A as 1 — Yes. In this example, there is an acute change of the resident’s behavior from alert and oriented as the family reported, to lethargic and incoherent during the interview.
Learn From C1310B Examples to Note Fluctuations
For sub-item C1310B — Inattention, the RAI Manual instructs you to assess attention separately from level of consciousness. Look for evidence of inattention during the resident interview, in the medical record, or from family or staff reports during the seven-day look-back period.
Tip: Another way to identify or confirm difficulty with attention is to ask the resident to count backwards from 20.
Example 1: During the BIMS interview, the resident wasn’t able to focus on all the questions asked and his gaze wandered. But several notes in the resident’s medical record indicate that he was attentive when staff communicated with him.
How to code: Here, you would code C1310B as 2 — Behavior present, fluctuates. You found evidence of inattention during the BIMS, but you noted that such evidence was absent in the medical record. This shows possible fluctuation in the behavior.
Example 2: You had to frequently repeat questions during the BIMS because the resident’s attention wandered. This behavior occurs throughout the interview, and medical records and staff agree that this behavior is consistently present. The resident also has a diagnosis of dementia.
How to code: Code C1310B as 1 — Behavior continuously present, does not fluctuate, because the resident’s attention consistently wandered throughout the seven-day look-back period. Note that the resident’s dementia diagnosis should not affect your coding here.
Don’t Code C1310C This Way When Resident Responds Incorrectly
The RAI Manual’s definition of “disorganized thinking” is “evidenced by rambling, irrelevant, or incoherent speech.” Although a resident’s answers to the BIMS could be wrong or inaccurate at times, this doesn’t necessarily mean that the resident’s thinking isn’t organized and coherent.
Example 1: The resident responds that the year is 1937 when you ask him to give the date. The medical record and staff indicate that the resident is never oriented to time, but he has coherent conversations. For instance, staff members report that he often discusses his passion for baseball.
How to code: Here, you would code C1310C — Disorganized thinking as 0 — Behavior not present. Even though the resident’s answer to the question was incorrect, it was related to the question. Also, no other sources reported disorganized thinking.
Example 2: You ask the resident (who is often confused) to give the date, and he responds with: “Let’s go get the sailor suits!” The resident continues to provide irrelevant or nonsensical responses throughout the interview. His medical record and the staff indicate that this is constant.
How to code: Code C1310C as 1 — Behavior continuously present, does not fluctuate, because all sources agree that the disorganized thinking is constant.
Example 3: The resident was able to tell you her name, the year, and where she was. She was able to talk about the activity she just attended, as well as the residents and staff who also attended. Then, the resident suddenly asks you, “Who are you? What are you doing in my daughter’s home?”
How to code: For this scenario, code C1310C as 2 — Behavior present, fluctuates, because the resident’s thinking fluctuated between coherent and incoherent at least once. Note that if as few as one source notes fluctuation, then you should code the behavior as 2.
Study 4 Definitions to Understand C1310D
For sub-item C1310D — Altered level of consciousness, the RAI Manual gives the following four types/definitions:
1. Vigilant — startles easily to any sound or touch;
Important: You don’t need a diagnosis of coma or stupor to code this behavior in C1310D.
Example 1: The resident is lying in bed. He arouses to soft touch but is only able to converse for a short time before his eyes close and he appears to be sleeping. Again, he arouses to voice or touch but only for short periods during the interview. Information from other sources (medical record, staff, and family) indicates that this was his condition throughout the look-back period.
How to code: Code C1310D as 1 — Behavior continuously present, does not fluctuate, because the resident’s lethargy was consistent throughout the interview and there is also consistent documentation of lethargy in the medical record during the look-back period.
Example 2: The resident is usually alert, as well as oriented to time, place and person. But today, at the time of the BIMS interview, the resident is conversant at the beginning but becomes lethargic and difficult to arouse thereafter.
How to code: Code C1310D as 2 — Behavior present, fluctuates, because the resident’s level of consciousness fluctuated during the interview. Remember that even if as few as one source notes fluctuation, you must code the behavior as 2.
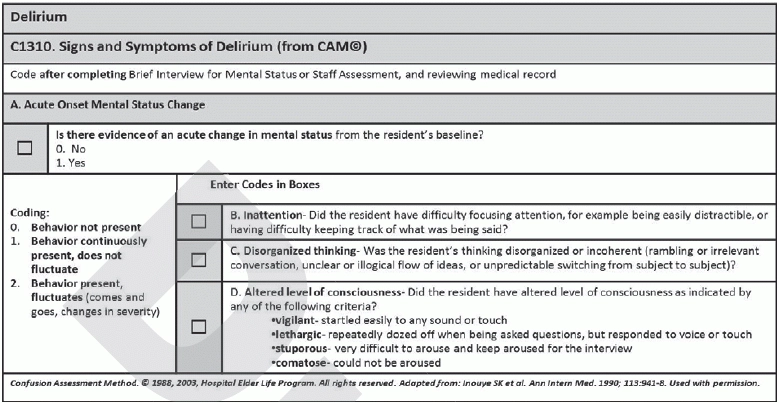
2. Lethargic — repeatedly dozes off when you are asking questions, but responds to voice or touch;
3. Stupor — very difficult to arouse and keep aroused for the interview; and
4. Comatose — cannot be aroused despite shaking and shouting.
