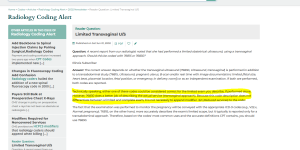
Hey guys this is to both of you for a limited 76830
say we do document imagining and print out images etc etc and we do a limited 76830 and document the element examined with documented images for an iud check or any reason the would be med necessary and do a lmitied 76830 what should i charge? would it be 76830 with mod 52 or i've even read to charge 76857 because despite it being a different approach 76857 has lower RVU's that might not be the current case as this was an older article in revenue cycle insider. I'm also attaching an image of some parameters i found for 76830 that mentions if evaluation of uterus is not performed or documented to use 52, but what if only 1 of those other sole components are performed and documented findings with also documented imaging could i charge 76380 with 52.
thank you so much
In reference to the IUD check this is what ACOG has published:
Use of Ultrasound
The performance of an ultrasound to check IUD placement is not bundled into the IUD insertion (code 58300), and it is not common
practice to use ultrasound to confirm placement. Therefore, this should not be routinely billed. However, ultrasonography may be used to confirm the location of the IUD when the qualified clinician incurs a difficult IUD placement (e.g., severe pain, uterine perforation, etc.). If ultrasound is used, one of the following codes is added:
Code 76857 Ultrasound, pelvic [nonobstetric], real time with
image documentation; limited or follow-up, or
Code 76830 Ultrasound, transvaginal
Occasionally, ultrasound is needed to guide IUD insertion. If ultrasound is used, add code 76998 (ultrasonic guidance, intraoperative).
But to answer your question, you would not bill a transabdominal ultrasound if a transvaginal one was performed. As to the use of modifier -52 that will be at the discretion of the payer (who may not recognize this modifier on code 76830) or the provider if the documentation simply indicates the IUD placement and mentions nothing else. The clinical vignette used to add this code to CPT is not very specific as to what is included:
intra service info: Supervise the sonographer performing the examination. The ultrasound examination, which may include evaluation of the uterus (including evaluation of the endometrium), ovaries, cul de sac, and parametrium, is interpreted. The examination results are compared and findings are correlated to previous studies. A report is dictated for the medical record.
Note the words "may include".
ACR, on the other hand, is very specific about the evaluation they expect when billing this code. I have always followed ACR on this matter as radiology, after all, is their specialty. I have always recommended using a modifier -52 on 76830 if the only documentation is IUD placement information and not an examination of the any of the uterine structures.
") thanks so much it seems clear that it's not between you and csperoni
thanks so much it seems clear that it's not between you and csperoni