- Messages
- 13
- Location
- Scott City, MO
I sent the following email to my providers and received one positive response and one negative response and one non response. Reaching out to get your thoughts on it.
"Good afternoon,
I wanted to go over these diagnoses with you.
M53.3 Sacrococcygeal disorders, not elsewhere classified
M46.1 Sacroiliitis, not elsewhere classified
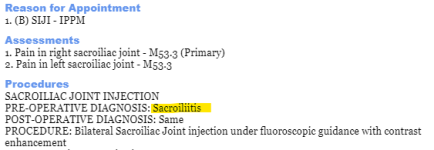
From the documentation on the Procedure note, it would seem that M46.1 would be the most appropriate code based on the Pre-Operative Diagnosis section stating "Sacroiliitis".
Also, the code does not need to be listed twice. I have to delete one of them on the claim because it creates an error. The codes themselves do not contain laterality. I've typed them above as they are listed in the ICD-10-CM book.
Please let me know what you think."
Negative Response:
"Hi everyone
I believe M53.3 (sacroiliac joint pain/disorder) is the correct icd 10 code, as this is the clinical diagnosis and syndrome we are treating with the joint injections
M46.1 - Sacroiliitis is a radiographic diagnosis identifying inflammation in the sacroiliac joints on imaging. If there is no imaging (CT or MRI) demonstrating inflammation in the joints, then this diagnosis is not appropriate. A patient can have sacroiliac joint pain (a clinical diagnosis) appropriately treated with a sacroiliac joint injection, without active sacroiliitis (M46.1)
Interested in hearing other thoughts/perspectives"
I reviewed his response last night and came across a website (https://my.clevelandclinic.org/health/diseases/17736-sacroiliitis) that indicates sacroiliitis is not just a radiographic diagnosis. Sacroiliac and Sacrococcygeal are two different structures.
Also, I'm not sure who put the dx codes in the system for them, but they do not match the description in our books.
"Good afternoon,
I wanted to go over these diagnoses with you.
M53.3 Sacrococcygeal disorders, not elsewhere classified
M46.1 Sacroiliitis, not elsewhere classified
From the documentation on the Procedure note, it would seem that M46.1 would be the most appropriate code based on the Pre-Operative Diagnosis section stating "Sacroiliitis".
Also, the code does not need to be listed twice. I have to delete one of them on the claim because it creates an error. The codes themselves do not contain laterality. I've typed them above as they are listed in the ICD-10-CM book.
Please let me know what you think."
Negative Response:
"Hi everyone
I believe M53.3 (sacroiliac joint pain/disorder) is the correct icd 10 code, as this is the clinical diagnosis and syndrome we are treating with the joint injections
M46.1 - Sacroiliitis is a radiographic diagnosis identifying inflammation in the sacroiliac joints on imaging. If there is no imaging (CT or MRI) demonstrating inflammation in the joints, then this diagnosis is not appropriate. A patient can have sacroiliac joint pain (a clinical diagnosis) appropriately treated with a sacroiliac joint injection, without active sacroiliitis (M46.1)
Interested in hearing other thoughts/perspectives"
I reviewed his response last night and came across a website (https://my.clevelandclinic.org/health/diseases/17736-sacroiliitis) that indicates sacroiliitis is not just a radiographic diagnosis. Sacroiliac and Sacrococcygeal are two different structures.
Also, I'm not sure who put the dx codes in the system for them, but they do not match the description in our books.