Hi, I wanted to ask if someone can provide me with some links or websites or anything really, that may have a list of common illnesses/injuries that are good examples to use for the different levels of the MDM table for Inpatient Hospital Coding (99221-99239)
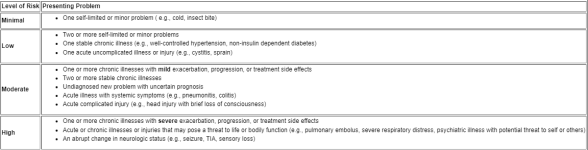
For example, just like on the Risk Table there's a row that says "Moderate" and has requirements like "Two or more stable chronic illnesses", what would a 'Stable Chronic Illness' be?
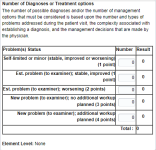
Also, I would LOVE some examples for the table that's for "Number of Diagnoses or Treatment options" I'm having a particularly hard time with this table when it comes to determining what problem is an established problem, and what's a new problem, and even when I know that it's a new problem most of the time I'm still not sure if it's a new problem with an additional workup plan or not.
I'm used to figuring out these questions mostly with 'Key Words' so if there's any kind of tips like that that I can use to make my coding a bit faster it'd be great.
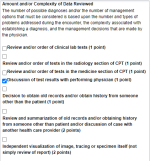
And for the "Data Reviewed table" I'd like to know what exactly does the "Discussion of test results with performing physician".
I'm a CPC-A coder, but I don't have a lot of experience so that's why I'm having some trouble with this.
Again, if anyone can provide me with a good long list of common illnesses/injuries that I can use for examples for the Risk table especially, I'd really appreciate it, thank you in advance.
AND/OR if you can give me a good explanation of your own, or direct me towards a good explanation of someone else about HOW I should be determining what problem is an established/new/new with additional workup etc. that would also be great.
I posted some pictures so it'll be easier.
For example, just like on the Risk Table there's a row that says "Moderate" and has requirements like "Two or more stable chronic illnesses", what would a 'Stable Chronic Illness' be?
Also, I would LOVE some examples for the table that's for "Number of Diagnoses or Treatment options" I'm having a particularly hard time with this table when it comes to determining what problem is an established problem, and what's a new problem, and even when I know that it's a new problem most of the time I'm still not sure if it's a new problem with an additional workup plan or not.
I'm used to figuring out these questions mostly with 'Key Words' so if there's any kind of tips like that that I can use to make my coding a bit faster it'd be great.
And for the "Data Reviewed table" I'd like to know what exactly does the "Discussion of test results with performing physician".
I'm a CPC-A coder, but I don't have a lot of experience so that's why I'm having some trouble with this.
Again, if anyone can provide me with a good long list of common illnesses/injuries that I can use for examples for the Risk table especially, I'd really appreciate it, thank you in advance.
AND/OR if you can give me a good explanation of your own, or direct me towards a good explanation of someone else about HOW I should be determining what problem is an established/new/new with additional workup etc. that would also be great.
I posted some pictures so it'll be easier.